

Names have been changed to protect patient privacy. Clinical details are shared with the patient’s consent.
When Nisha first called us, she didn’t come with a long list of questions. She came with exhaustion.
She said something very simple: “I’ve tried everything… I don’t know what else to do.”
Nisha was 26, married for about 1.5 years, and had been trying to conceive. She worked as an advocate, a demanding profession that left little room for the kind of careful self-care her body needed. She had been dealing with PCOS since puberty, with irregular periods for as long as she could remember.
For more on this, read our guide on Lean PCOS. This is her story, from that first defeated phone call to a positive pregnancy test.
The Situation
Nisha’s profile painted a picture we see often in our clinic: a young woman who is trying hard but not getting the guidance she needs.
Nisha’s profile:
- Age: 26
- Weight: 100 kg
- AMH: 8.56 ng/mL (elevated, a hallmark of PCOS)
- Diagnosis: PCOS since puberty + hypothyroidism
- Periods: Irregular since adolescence, often absent for months
- Previous treatment: Multiple ovulation induction (OI) cycles, ovulated, but no pregnancy
- Family history: Mother with PCOS and thyroid issues, cousins with PCOS
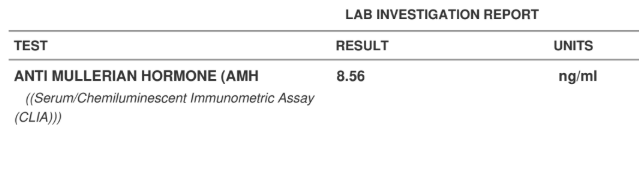
Her AMH of 8.56 ng/mL is a classic PCOS marker. Unlike low AMH (which indicates fewer eggs), a high AMH in PCOS typically reflects a large number of small follicles that aren’t maturing properly. The ovaries are producing follicles, but none of them are reaching ovulation, which is why her cycles were irregular despite having plenty of eggs (Dewailly et al., 2011, Human Reproduction Update).
She also had hypothyroidism, but because of stress and repeated disappointment from fertility treatments, she had stopped taking her thyroid medication regularly. Untreated hypothyroidism further disrupts ovulation and makes PCOS harder to manage (Singla et al., 2015, Indian Journal of Endocrinology and Metabolism).
There was also a strong genetic component. Her mother had both PCOS and thyroid issues. Her cousins had PCOS. Somewhere along the way, Nisha had started believing: “Maybe this is just my body. Maybe this won’t change.”
What stood out to us immediately: Nisha wasn’t someone who wasn’t trying. She told us, “I’m going to the gym… I’m trying to eat better… but nothing is working.” That frustration (when effort doesn’t match results) was the hardest part for her.
📞 Does This Sound Like Your Story?
If you’ve been dealing with PCOS and trying to conceive without success, a personalised assessment can help identify what’s being missed.
What We Found
In our first few interactions, we spent time understanding Nisha’s full story, not just her reports, but her daily life, her eating patterns, her movement, her stress, and her emotional state.
1. PCOS and hypothyroidism were not being managed together
This is something we see frequently. Nisha was being treated for PCOS (ovulation induction) by her gynaecologist, and had thyroid medication prescribed separately, but nobody was looking at the two conditions as an interconnected system. PCOS and hypothyroidism share overlapping metabolic pathways, managing one without the other is like treating half the picture (Sinha et al., 2020, Frontiers in Endocrinology).
2. Good effort, but no structure
Nisha was going to the gym. She was trying to eat better. But “trying to eat better” without a clear plan often means well-intentioned but inconsistent choices. She didn’t know what a balanced plate for PCOS actually looked like, or how meal timing affected her insulin levels.
3. The focus had been only on ovulation, not the underlying environment
Her previous treatment cycles focused on forcing ovulation through medication. But ovulation is the end result of a complex hormonal cascade. If the underlying environment, insulin sensitivity, inflammation, thyroid function, cortisol, isn’t addressed, even successful ovulation doesn’t guarantee conception (Teede et al., 2018. International Evidence-Based PCOS Guidelines).
In one of our early discussions, Nisha asked: “If I’m already doing so much… why is my body not listening?”
That’s where we explained: it’s not about doing more. It’s about doing the right things, in the right way, consistently.
Once she understood this, there was a visible shift, not just in what she did, but in how she approached her own body.
The Plan
We were very clear from the beginning: this is not going to be an aggressive or extreme plan.
In fact, one of the first things we told Nisha was: “You don’t have to do more. You just have to do it differently.”
Nutrition. Structure Over Restriction
Our nutritionist worked closely with Nisha on meals, not just giving her a diet chart, but helping her understand what to eat and why.
The focus was on:
- Balanced plates: protein, complex carbs, vegetables, and healthy fats at every meal
- Meal timing: consistent eating schedule to stabilise insulin (insulin resistance is a core driver of PCOS)
- Indian foods she could actually cook: brown rice, dals, paneer, vegetables, eggs. No exotic superfoods.
- No deprivation: Nisha had tried restriction before and it hadn’t worked. Nourishment was the approach.
There were days she would message: “Is this plate okay?” And the team would guide her, small corrections, not overwhelming changes.


Movement. Consistent, Not Extreme
Nisha was already going to the gym, so we didn’t push harder workouts. We aligned her existing activity with consistency and recovery. The goal was daily movement she could sustain, not intense sessions she’d burn out from.
- Walking 10,000+ steps daily
- Gym sessions aligned with her energy levels
- Recovery days built in, no guilt about rest days
Thyroid Management
We emphasised the importance of taking her thyroid medication consistently. This wasn’t our prescription (it was her existing doctor’s) but she needed to understand why skipping it was undermining everything else she was doing.
Emotional Support
Regular check-ins with the team. This wasn’t just about meal plans. Nisha needed someone to tell her, “This is working. Don’t rush the process.”
It was a very collaborative process, not instructions, but guidance.
The Journey
Week 1: The First Signs
Nisha started noticing changes almost immediately:
- Better energy
- Feeling lighter
- A visible glow after workouts
She shared her post-workout photos, and her message that week said it all:
“It has been a week and I can actually sense a change in my lifestyle and health. The diet is so fulfilling and the amazing part is, it is very easy to make. I really appreciates the exercises you share everyday. It makes my body refreshing and active.”
(For the types of movement we recommend for PCOS, see our guide on PCOS exercise: what actually helps.)
She was hitting 11,000+ steps daily:

We told her: “This is your body responding. Keep going.”
Month 1: The Breakthrough
This was a big emotional moment.
Nisha got her period, naturally, without medication, on a proper cycle.
For someone who had irregular or absent periods since puberty, this wasn’t just a cycle. It was the first time her body felt “normal.”
At the same time, she lost 3 kg:
There were also struggles. Some days she felt impatient. Some days she wanted faster weight loss. We had regular conversations reassuring her: “This is working. Don’t rush the process.”
Months 2-3: Building Confidence
Nisha became more confident. Her plates became more consistent. She stopped asking “Is this right?”. She knew what to do.
Her step count kept climbing:

By the end of 3 months:
- ~8 kg weight loss (100 → ~92 kg)
- Better cycles: periods becoming more regular
- More stable energy and improved mood
At the end of the programme, she told us: “I finally understand my body.”
Her final message at the end of 3 months was deeply meaningful to our team:
“Thank you so much guys… Thanks to Subi for your kind words and motivation… Actually, like Dr Suganya suggested, I am going to give myself 3 more months to take care of my body… you have changed my way of eating… I am still going to follow your diet and will update you on my weight loss.”
That last line was everything. She wasn’t dependent on us anymore. She was continuing the plan on her own, which is always our goal.
After the Programme
What happened next is what makes this case study special.
Nisha didn’t just maintain. She continued independently. And she kept us updated.
Month 4: Continued Progress
A few months after the programme ended, she messaged:
“I have been following your diet with exercise and now I have lost around 8.5 kgs. My follicles started growing just on Letrozole without injection… I’m confident that it’ll happen too. Thank you so much for your guidance.”
This is an important detail. A year earlier, Nisha had undergone ovulation induction with injections, and even though she ovulated, nothing happened. Now, after the lifestyle changes, her body was responding to Letrozole alone, without injections. Her gynaecologist was doing her part, and the lifestyle work had made Nisha’s body more receptive to minimal medication.
This is exactly how we believe fertility care should work: lifestyle optimisation supporting medical treatment, not replacing it. Nisha’s gynaecologist handled the medical side. We added the lifestyle layer. Together, it worked.
Month 5: The Moment
And then came the message. Short. Simple. But very special.
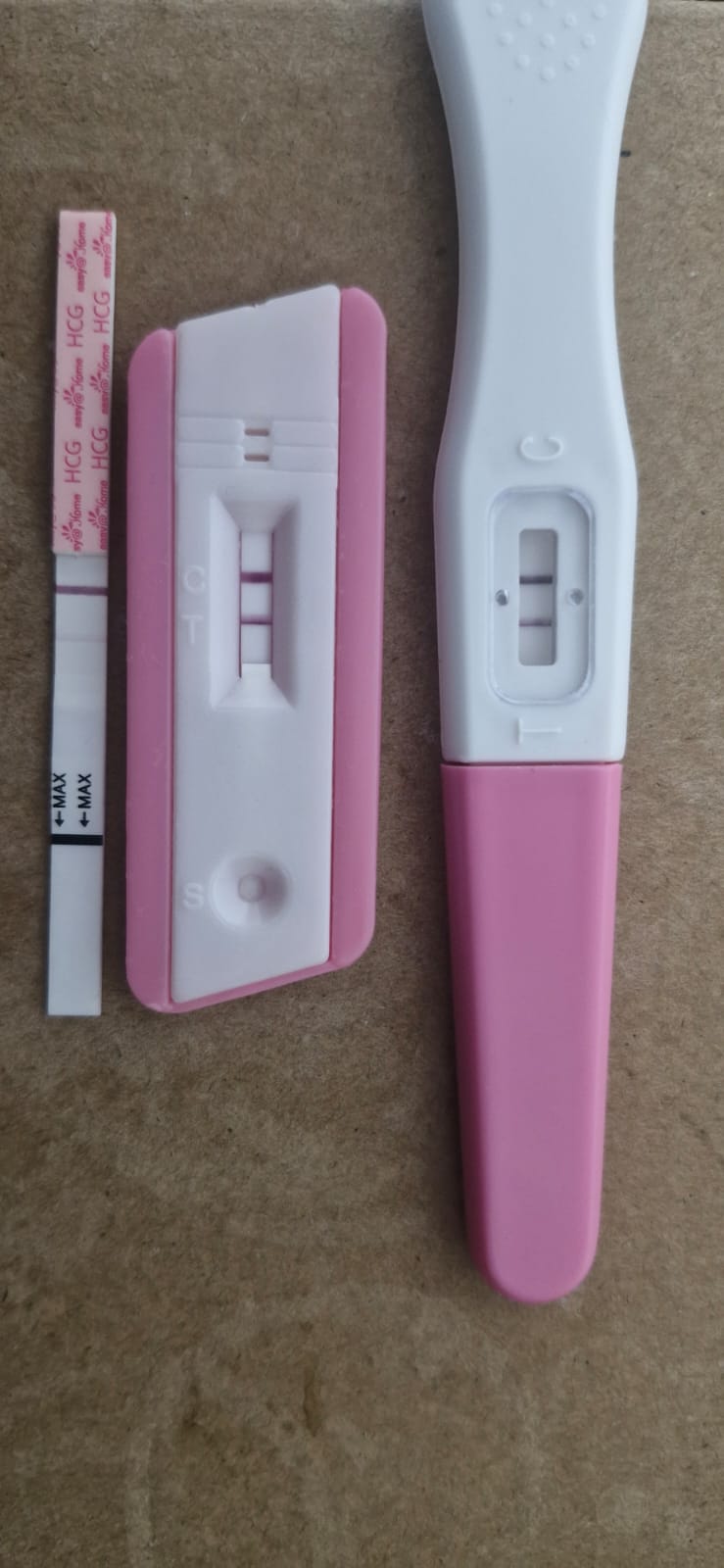
She had conceived. On Letrozole alone. No injections. No IVF.
Her detailed update, shared in her own words:
“I joined Fertilia in June 2025 for three months. I still continue to follow the diet pattern suggested by Dr Suganya Fertilia till today. One additional thing I did was start going to the gym. Both of these helped me lose weight.
Earlier, I had no periods. After regularising my diet, I got random periods. Over the last three months, my cycle became more regular and settled around 34 days.
About a year ago, I underwent ovulation induction (OI) treatment. Even though I ovulated then, nothing happened. In the last three months, I was on Letrozole, and yesterday I found this.
I’m still a little scared about how things may go forward, but for now I’m feeling grateful and content.
A big thank you to everyone @Dr Suganya Fertilia @Elakiya @Riya for the support and encouragement throughout this journey.”
The Outcome
| Metric | Before | After (5 months) |
|---|---|---|
| Weight | 100 kg | ~91 kg (−9 kg) |
| Periods | Absent / irregular since puberty | Regular 34-day cycles |
| AMH | 8.56 ng/mL (elevated) | , (not retested) |
| Ovulation | Only with injections | Spontaneous on Letrozole alone |
| Previous OI | Failed despite ovulating | , |
| Pregnancy | 1.5 years of trying, no success | Conceived |
From lifelong irregular cycles, PCOS since puberty, failed ovulation treatments, and 100 kg, to regular periods, 9 kg lost, and a positive pregnancy test.
💜 Dealing with PCOS and Trying to Conceive?
Every woman’s PCOS is different. What worked for Nisha was a plan designed specifically for her body, her lifestyle, and her medical history. A personalised assessment can help you understand what your body needs.
What This Case Study Teaches Us
1. PCOS is reversible with the right approach
PCOS is not a life sentence. The symptoms (irregular periods, weight gain, difficulty conceiving) are driven by underlying metabolic factors that respond to structured lifestyle changes. A 2019 review in Nature Reviews Endocrinology confirmed that lifestyle modification is the first-line treatment for PCOS, particularly when insulin resistance is a driver (Teede et al., 2018).
Nisha’s periods returned within one month of starting the programme, without medication. Her body was capable of ovulating; it just needed the right metabolic environment.
2. High AMH in PCOS isn’t “good”. It’s part of the problem
Many women with PCOS see a high AMH and think: “At least I have lots of eggs.” But elevated AMH in PCOS reflects follicular arrest, too many follicles competing, none of them maturing to ovulation (Dewailly et al., 2011). The goal is to create the hormonal and metabolic conditions where one dominant follicle can emerge and ovulate. That’s what happened with Nisha.
3. Lifestyle changes don’t replace medical treatment. They make it work better
Nisha’s gynaecologist prescribed Letrozole. Our programme prepared her body to respond to it. A year earlier, she’d had ovulation induction with injections and still didn’t conceive. After 3 months of structured nutrition and movement, her follicles responded to Letrozole alone, no injections needed.
This is the model we believe in: your gynaecologist handles the medical treatment, and we add the lifestyle foundation that makes treatment more effective. One doesn’t replace the other. (Related reading: How to Track Ovulation: Indian Woman’s Guide)
4. Structure beats effort
Nisha was already going to the gym before she came to us. She was already trying to eat better. But effort without structure is like driving without a map. Once she had a clear nutrition plan, consistent meal timing, and the right balance of macronutrients, her body started responding. The amount of effort didn’t change, the direction did.
5. The real win is independence
The most telling part of Nisha’s story isn’t the pregnancy test. It’s this line from her end-of-programme message: “I am still going to follow your diet.” She didn’t need us anymore. She had learned how her body worked, what it needed, and how to give it that consistently. That’s the outcome we optimise for. (Also see: PCOS Belly: Why It Happens & How to Reduce It)
Frequently Asked Questions
Can PCOS really be “reversed”?
PCOS can’t be cured. It’s a chronic condition with a genetic component. But its symptoms (irregular periods, weight gain, acne, hair growth, difficulty conceiving) can be significantly improved or resolved through lifestyle changes that address the underlying drivers: insulin resistance, chronic inflammation, and hormonal imbalance. When people say “PCOS reversal,” they mean symptom resolution, and yes, that’s absolutely achievable. Nisha’s periods returned within one month. (For more on PCOS symptoms, see: PCOS Hair Growth: Why It Happens & What Works)
What does a high AMH mean for fertility?
In the context of PCOS, a high AMH (typically above 4.5–5.0 ng/mL) indicates an excess of antral follicles. This doesn’t mean you have “better” fertility, it means your ovaries are producing many follicles that aren’t maturing properly. The clinical challenge is helping one follicle become dominant and ovulate. Lifestyle changes that improve insulin sensitivity can help normalise this process (Dumont et al., 2015, Reproductive Biology and Endocrinology).
How much weight do you need to lose for PCOS to improve?
Even a 5–7% reduction in body weight can significantly improve ovulation rates, menstrual regularity, and conception chances in women with PCOS (Kiddy et al., 1992, Clinical Endocrinology; Clark et al., 1998, Human Reproduction). Nisha lost about 9% of her body weight (100 → 91 kg), which falls in this range. The key is sustainable loss through nourishment, not crash dieting.
Should I stop my fertility medication and try lifestyle changes instead?
No. please don’t stop any prescribed medication without consulting your doctor. Lifestyle optimisation works best alongside medical treatment, not instead of it. In Nisha’s case, lifestyle changes made her body responsive to a lower dose of medication (Letrozole alone, no injections). Continue working with your gynaecologist, and add structured lifestyle support to maximise your chances.
How long does it take for lifestyle changes to help with PCOS?
Most women start seeing menstrual improvements within 1–3 months of consistent lifestyle changes. Ovulation can improve within 2–3 cycles. Nisha got her first natural period within Month 1 and conceived by Month 5. For women actively trying to conceive, our guide on how to get pregnant naturally covers the timing, nutrition, and lifestyle steps that complement PCOS treatment. However, every woman’s timeline is different, it depends on the severity of PCOS, presence of other conditions (like hypothyroidism), starting weight, and consistency with the plan.
What’s different about Fertilia’s approach to PCOS?
We don’t just treat the symptoms. We connect the dots. PCOS rarely exists in isolation. Nisha had PCOS + hypothyroidism + insulin resistance + a strong genetic component. Our programme addresses all of these together, with a personalised nutrition plan (designed by a nutritionist who understands PCOS), movement guidance, thyroid management support, and regular emotional check-ins. Your gynaecologist manages the medical treatment; we add the lifestyle foundation. It’s a team approach.
This is the second in our series of patient case studies. Every story is real, verified, and shared with the patient’s consent. Names and identifying details are changed to protect privacy.
Dr. Suganya Venkat is an OB-GYN with 15+ years of experience. She holds an MBBS (SRMC, 5 Gold Medals), MD in Pathology (CMC Vellore), and DNB in OB-GYN (GKNM Hospital, Coimbatore).



