

Name has been changed to protect patient privacy. Clinical details and images are shared with the patient’s consent.
When Sujatha reached out to us, she didn’t have the “typical” PCOS story.
She wasn’t overweight. She didn’t have dramatic symptoms that anyone could see from the outside. At 53.3 kg and 164 cm, her body looked perfectly fine on paper.
But she had never (not once in her life) had a menstrual period without taking a tablet first.
She was 22, an engineering student living in a hostel, and she was exhausted. Not from her studies, but from years of visiting hospitals, getting prescribed the same tablets over and over, and never understanding why her body wouldn’t do what it was supposed to do on its own.
“I’ve been to so many doctors… they all say the same thing, take this tablet, come back next month.”
That cycle of hope and disappointment had worn her down. By the time she found Fertilia, the exhaustion wasn’t just physical. It was emotional, a quiet loss of confidence in her own body.
Going Deeper: What the Full Assessment Revealed
Sujatha’s ultrasound told part of the story:
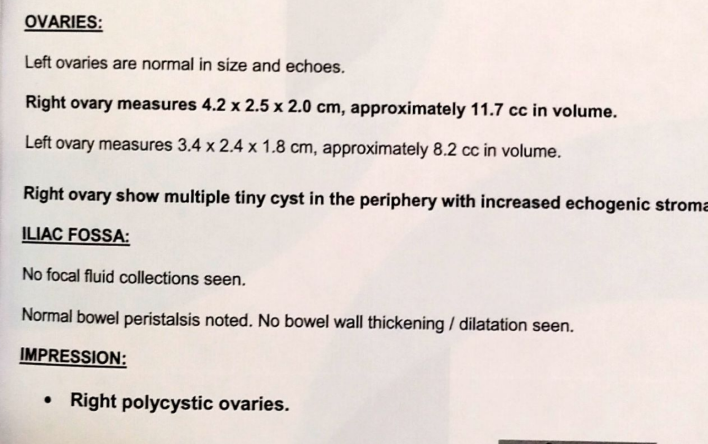
Right polycystic ovaries. Multiple tiny cysts along the periphery. Increased echogenic stroma. This is a textbook ultrasound finding in PCOS.
But here’s what made her case different: she was lean.
Most PCOS awareness focuses on weight gain, insulin resistance in overweight women, and the advice to “just lose weight.” When you’re already at a healthy BMI, that advice doesn’t feel relevant. And in busy outpatient settings, a normal BMI can sometimes mean the deeper investigation doesn’t happen, not because of negligence, but because lean PCOS simply isn’t as well recognised yet.
At Fertilia, we ran the full panel.
Sujatha had lean PCOS: a presentation where the body appears healthy from the outside, but hormonally and metabolically, the picture is very different. (If you’re not familiar with the different ways PCOS can present, our PCOS: Symptoms, Root Causes & Treatment guide covers the full picture.) Although she looked lean, she had visible fat accumulation around her abdomen and facial hair growth, classic signs of androgen excess that had nothing to do with her scale weight.
When we ran her full panel, the results told us exactly what was going on beneath the surface:
Elevated hs-CRP. Chronic Inflammation
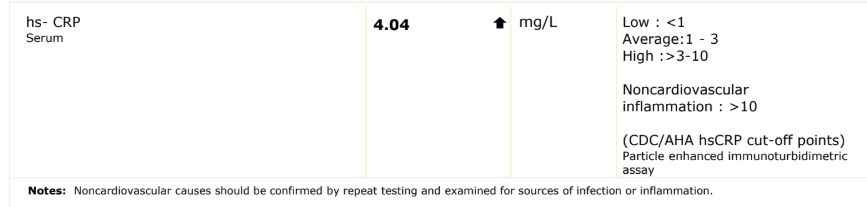
Her hs-CRP was 4.04 mg/L. According to the CDC/AHA cardiovascular risk classification used on her report, values below 1 are low risk, 1–3 are average, and above 3 are elevated. Hers was in the high range, indicating chronic, low-grade inflammation. This is one of the recognised PCOS drivers: inflammation disrupts ovarian function and worsens androgen production, even in women who are not overweight. (We cover this mechanism in detail in our Insulin Resistance & PCOS guide.)
Low Vitamin D. Deficient
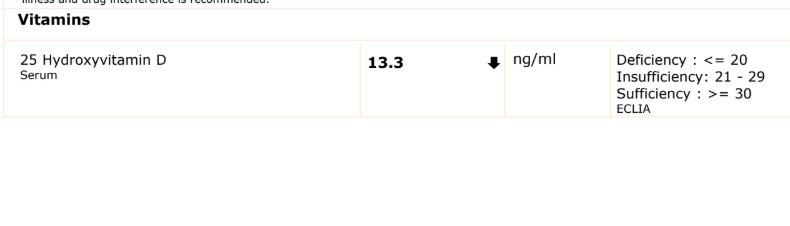
Her 25-Hydroxyvitamin D was 13.3 ng/ml. Deficiency is defined as ≤20 ng/ml. Sufficiency starts at 30. Vitamin D deficiency is extremely common in Indian women and has been directly linked to worsening insulin sensitivity and hormonal imbalance in PCOS, even in lean women.
For more on this, read our guide on When PCOS Starts at 15.
Low Vitamin B12. Contributing to Fatigue
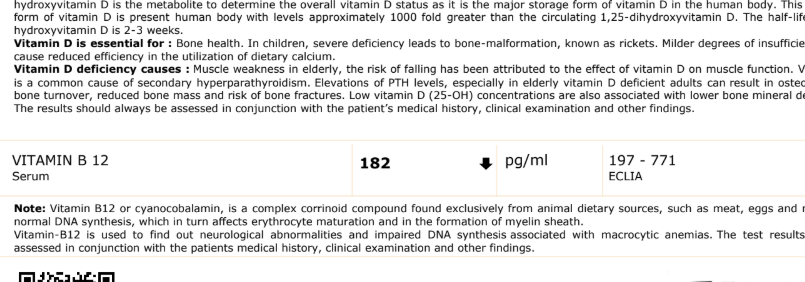
Her B12 was 182 pg/ml: below the reference range of 197–771. This was contributing to her fatigue and metabolic inefficiency. For a young student managing a demanding academic schedule, this deficiency alone was silently draining her energy.
This is what structured, evidence-based assessment looks like. Instead of another round of tablets to force a period, we identified the actual drivers, inflammation, nutritional deficiencies, and hormonal imbalance, and built a plan around correcting them.
The Weight Confusion That Made Things Worse
Before joining Fertilia, Sujatha had tried to fix things on her own. She’d heard that low body weight could be a reason for absent periods. So she started eating more, mostly hostel food and outside food, because that’s what was available.
Within 3 months, she gained nearly 6 kg. Her periods still didn’t come.
Then the opposite happened. She rapidly lost 5 kg in a single month. These extreme fluctuations further destabilised her hormones, shattered her confidence, and deepened her fear around food.
This is a pattern we see often with lean PCOS. Women either don’t think they need lifestyle changes because they’re “not fat,” or they swing between extremes because no one has explained what their body actually needs. Sujatha didn’t need to gain weight or lose weight. She needed the right nutrition to correct specific deficiencies and reduce inflammation.
For more on this, read our guide on PCOS Is Now PMOS.
If you’re dealing with irregular periods or PCOS and aren’t sure what’s really going on, Dr. Suganya can help you understand your body better. Talk to Dr. Suganya on WhatsApp →
The Plan: Making It Work in a Hostel
This was the real challenge. Sujatha wasn’t living at home with a kitchen and family support. She was in a college hostel with:
- Limited food choices (whatever the hostel served that day)
- No kitchen access
- A hectic academic schedule
- Constant temptation of outside food with friends
A complicated diet plan would have failed on Day 1. So we built something different, a plan designed around her real life, not an ideal one.
First: Correct the Deficiencies
No amount of diet tweaking would have worked without addressing the foundations. We started with:
- Clinically appropriate Vitamin D correction: targeted supplementation to get from 13.3 to above 30
- Active B12 supplementation: to restore energy and metabolic function
- Anti-inflammatory food pattern: not a restrictive diet, but a shift in the quality of what she ate (similar principles to our PCOS Diet Chart)
Then: The Hostel Hacks
Instead of telling her what she couldn’t eat, we focused on what she could add, even within hostel constraints.
The kettle strategy:
We started with one simple tool, a small multipurpose kettle in her room. It sounds small, but it changed everything.
With the kettle, she could boil eggs. This meant that no matter what the hostel served, she had at least one reliable source of protein alongside her meal.

Over time, we introduced soaked and cooked pulses using the same kettle. On days when the hostel menu was completely junk, she had a backup, just boil some moong or chana and have a nourishing protein-rich option without depending on outside food.

The millet mix:
For busy days (exams, lab sessions, early morning classes) we introduced a meal-replacement millet mix. Easy to prepare, nutritionally dense, and it gradually replaced her dependence on outside food.

Infused water with basic spices:
We guided her to keep a few spices in her room, jeera, pepper, cinnamon. Using these, she could prepare infused water that gently supported her metabolism throughout the day. She also made an effort to include fruits and seeds whenever possible.

Nothing here was extreme. Nothing was overwhelming. Just small, thoughtful changes that fit into a 22-year-old’s real life in a college hostel.
Because real transformation doesn’t come from perfect plans. It comes from simple habits you can actually follow every single day.
What Changed. Month by Month
Month 1: The First Natural Period
From the very first month, Sujatha followed the plan as best as she could. Supplements regularly. Balanced meals when possible. Walking when her schedule allowed. Some days she managed a workout, some days she couldn’t.
There were moments of doubt. “Am I doing this right? Is this enough? Why isn’t my body responding faster?”
But she chose consistency over perfection.
And then, within just one month, she got her menstrual period naturally. Without a single tablet.
It might sound like a small thing to someone who’s never struggled with this. But for a woman who had never experienced a natural cycle in her life, it felt like everything.
The cycle came two days later than her previous tablet-induced period. The flow was lighter. For a moment, she wasn’t sure what to feel, happy, confused, slightly worried.
But deep down, it meant one important thing: her body was starting to respond on its own.
Month 2: Confirmation
She continued the same routine. Not perfectly, but consistently. There were still ups and downs, days when motivation came easily and days when it didn’t.
The result:
- Periods arrived on time, naturally
- Flow was normal
- Abdominal fat reduced, her midsection felt more balanced and comfortable
- Overall hormonal rhythm and metabolic response improved
This steady progression was reassuring in its own quiet way. No forcing. No pushing beyond limits. Just consistent, supportive changes, and her body responding.
After the Program: Still Going
This is the part that mattered most.
Even after her program ended, Sujatha got her periods naturally the following month. No reminder, no intervention, just her body continuing to stay in rhythm.

It wasn’t just about getting her cycle back. It was about knowing that her body could sustain it.
In Her Own Words
After completing the program, Sujatha shared her experience:
And her Google review:
Why Lean PCOS Gets Overlooked
Sujatha’s story carries an important message that we want every woman reading this to hear:
PCOS is not just a “weight problem.”
Women with lean PCOS are often told there’s nothing wrong because their BMI is normal. They’re told to “just wait” or given tablets without any investigation into why their cycles aren’t working.
But lean PCOS is real, and it needs the same structured, personalised approach as any other presentation. The drivers may be different, inflammation, nutritional deficiencies, adrenal androgen excess, but the need for targeted correction is the same.
What Sujatha’s case proved:
- You don’t have to be overweight to have PCOS that needs active management
- Lifestyle modifications matter for lean PCOS just as much as for the overweight presentation: but they need to be different modifications, targeted to your specific drivers
- Practical, sustainable changes beat extreme plans: especially for young women managing studies, hostel life, and limited resources
- The right supplements without the right lifestyle won’t work. The right lifestyle without correcting deficiencies won’t work either. It’s the combination that makes the difference.
Whether you have lean PCOS or classic PCOS, every woman deserves a plan built for her body, not a generic prescription. Dr. Suganya works with each patient individually, starting with a thorough assessment of what’s actually going on. Start a conversation with Dr. Suganya on WhatsApp →
Frequently Asked Questions
What is lean PCOS?
Lean PCOS refers to polycystic ovary syndrome in women who have a normal or low BMI (below 25). The hormonal and metabolic imbalances, irregular periods, androgen excess, insulin sensitivity issues, are present, but without the visible weight gain that most people associate with PCOS. Studies estimate that roughly 20–30% of women with PCOS may fall into the lean category (Veltman-Verhulst et al., 2012; prevalence varies by population and diagnostic criteria used).
Can you have PCOS without being overweight?
Yes. PCOS is a hormonal and metabolic condition, not a weight condition. While many women with PCOS do experience weight gain, lean women can have the same hormonal disruptions, irregular or absent periods, elevated androgens (causing facial hair or acne), and polycystic ovaries on ultrasound. The key drivers in lean PCOS are often inflammation, adrenal androgen excess, and nutritional deficiencies rather than insulin resistance alone.
Do women with lean PCOS need lifestyle changes?
Absolutely. This is one of the most common misconceptions. Because they’re already at a healthy weight, many lean PCOS patients (and sometimes their doctors) assume lifestyle modifications aren’t needed. But the right nutrition, targeted supplementation, anti-inflammatory eating patterns, and consistent movement can directly address the underlying drivers. Sujatha’s case is a clear example: she was 53 kg and still needed specific dietary and supplementation changes to get her cycles back.
Can PCOS periods return without medication?
In many cases, yes. When the underlying drivers, whether that’s inflammation, nutritional deficiencies, insulin resistance, or a combination, are properly identified and addressed through lifestyle, nutrition, and targeted supplementation, the body’s hormonal rhythm can restore itself. This doesn’t happen overnight, and it doesn’t happen with generic advice. It requires a personalised approach. Sujatha got her first natural period in Month 1 and sustained it after the program ended.
How do you manage a PCOS diet plan in a hostel?
This was one of the biggest challenges in Sujatha’s case, and it’s a question we hear from many students. The key is working with the constraints, not against them. Practical strategies include: keeping a small kettle for boiling eggs and pulses (reliable protein sources), using a millet-based meal mix for busy days, keeping basic spices for infused water, and adding protein alongside whatever the hostel serves rather than trying to replace it entirely.
Is abdominal fat in lean PCOS different from regular belly fat?
Yes. Women with lean PCOS can accumulate fat specifically around the abdomen (central adiposity) even while maintaining normal overall body weight. This fat distribution is driven by hormonal factors (particularly androgen excess and cortisol) rather than simple caloric surplus. It’s one of the clinical signs that distinguishes lean PCOS from a truly healthy metabolic state, and it often responds well to anti-inflammatory nutrition and targeted lifestyle changes.
Should I see a doctor for lean PCOS or can I manage it on my own?
A thorough medical assessment is essential. As Sujatha’s case shows, the underlying drivers (inflammation, vitamin deficiencies, hormonal imbalances) need proper investigation through blood work and ultrasound. They can’t be guessed at from symptoms alone. Once you know what’s actually going on, the lifestyle plan can be targeted and effective. Without that assessment, you risk the same trial-and-error cycle that Sujatha experienced before joining the program.
This is the fourth in our series of patient case studies from our clinic. Every story is real, verified, and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.



