

Name changed to protect patient privacy. Clinical details shared with her consent.
When Gowri first reached out, she didn’t come to us on her own. Her fertility doctor sent her to Fertilia.
That part of the story matters, because it’s increasingly how we meet patients. Another doctor, a gynaecologist planning a fertility cycle, looks at the reports, looks at the person in front of her, and says: “Let’s get you ready before we start treatment. Go see Dr. Suganya first to prep your body before treatment.”
Gowri was 30. Married. Had been trying to conceive, and it wasn’t happening. Her reports told part of the story. Her body told the rest.
This is how 3 months of preparation changed what was possible for her.
The Situation
By the time Gowri came to us, she had been carrying the weight (literal and emotional) of fertility struggle for a long time.
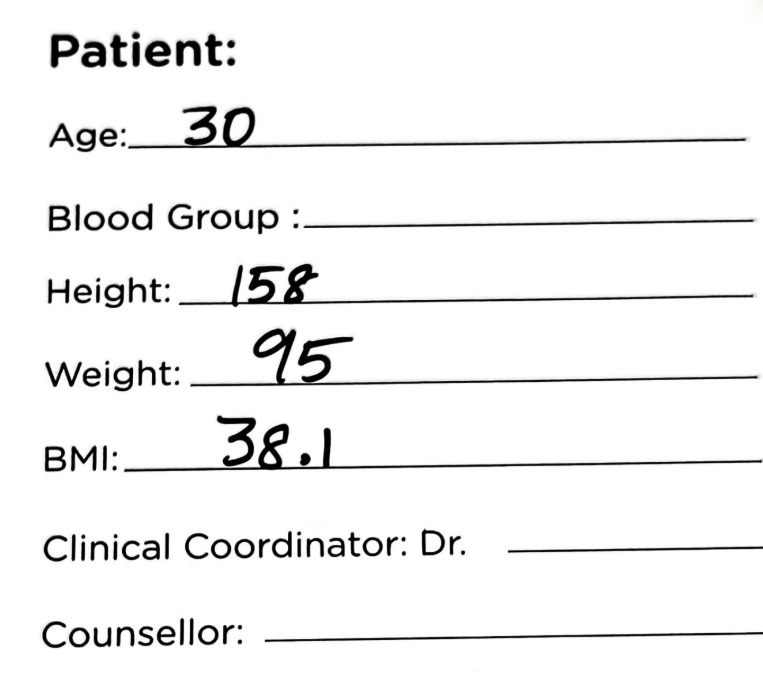
Gowri’s profile:
- Age: 30
- Height: 158 cm
- Starting weight: 95 kg
- BMI: 38.1 (obesity category)
- Diagnosis: PCOS (known since college years)
- Periods: Irregular since adolescence
- HbA1c: 9.8% (diabetic range; anything above 6.5% is clinically diabetes)
- Estimated average glucose: 234 mg/dL (normal is 70–126)
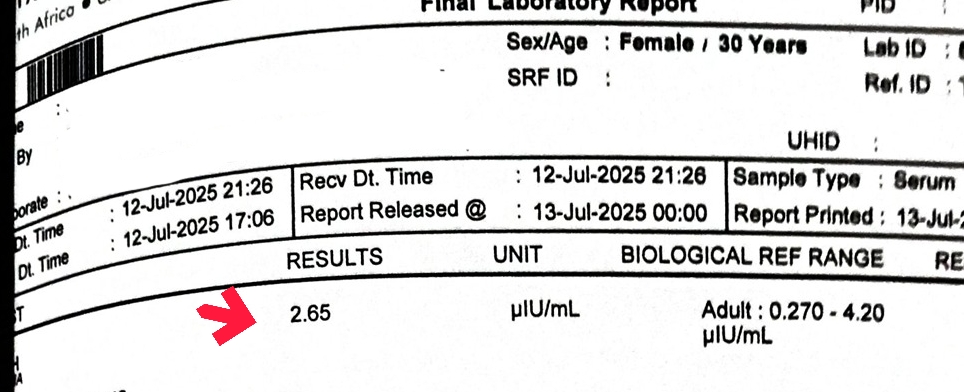
- TSH: 3.21 µIU/mL (within the adult lab range of 0.27–4.20 but above the preferred pre-conception target of <2.5)
- Acanthosis nigricans: present (darkened, velvety skin on the neck and underarms, a clinical marker of severe insulin resistance)
- Body composition: significant central (belly) weight gain, a hallmark of insulin-driven PCOS
- TTC duration: long, described as “a major emotional concern” after marriage
- Previous attempts: multiple diets, multiple approaches, nothing sustainable
- Referred by: her gynaecologist, for hormonal balancing and preconception preparation before starting fertility treatment
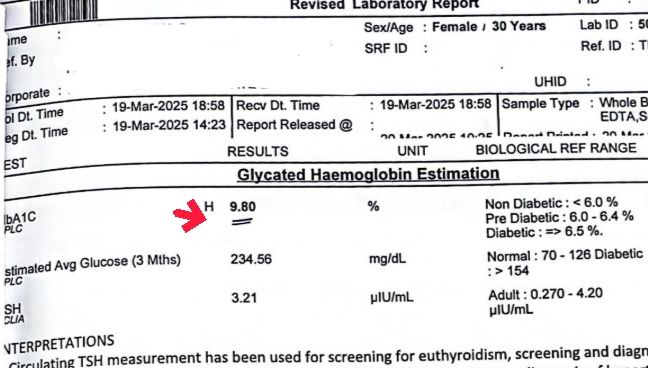
That HbA1c of 9.8% is not a mild deviation. It reflects poor glucose control over the prior three months and puts her squarely in uncontrolled type 2 diabetes territory. Combined with her PCOS, her BMI of 38, and clinical acanthosis nigricans, she had what we’d clinically call severe metabolic dysfunction. Not one problem. A whole cluster.
In that state, pregnancy isn’t just harder to achieve. When it does happen, it carries significantly higher risks of miscarriage, congenital anomalies, gestational diabetes, and preterm birth. Her gynaecologist understood this. That’s why she was sent to us before anything else was started.
Before we explained any plan, Gowri said something we hear often:
“I’ve tried so many diets before. Nothing stays.”
She wasn’t wrong. She had tried hard. The problem wasn’t her effort. It was that nobody had looked at her whole picture together.
📞 Is Your Doctor Suggesting Lifestyle Changes Before Fertility Treatment?
If your gynaecologist has asked you to work on your weight, blood sugar, or PCOS before starting IUI or IVF, you’re not being delayed, you’re being set up to succeed. A personalised assessment can help you use this window well.
What We Found
When we sat down with Gowri and her reports, three things became clear very quickly.
1. Her PCOS was being driven primarily by insulin resistance
PCOS is one condition with multiple drivers. In Gowri’s case, the driver was loud: central adiposity, acanthosis nigricans, HbA1c 9.8%, and a long history of belly weight gain that she couldn’t shift. This is classic insulin-driven PCOS (Dunaif, 1997, Endocrine Reviews). Treating her PCOS without first addressing her metabolic state would have been treating the symptom and ignoring the engine.
(Related reading: Insulin Resistance and PCOS: Signs, Diet, and What to Do)
2. Her HbA1c needed to come down before pregnancy, not during
Guidelines for women with diabetes or prediabetes who are trying to conceive are clear: aim for HbA1c below 6.5% (ideally below 6.0%) before pregnancy. The reason is clinical, not cosmetic. Higher HbA1c in early pregnancy is associated with sharply higher rates of miscarriage and congenital anomalies (Xodo et al., 2021, Medicina; BMC Pregnancy and Childbirth, 2025). Getting pregnant at 9.8% would have been unsafe even if it had happened.
3. Her thyroid was “normal” on paper but not optimal for fertility
Her TSH of 3.21 is within the standard adult reference range. But for a woman trying to conceive, the preferred target is usually below 2.5 µIU/mL. Subtle thyroid issues can disrupt ovulation and raise miscarriage risk even when the lab flag is not red (Singla et al., 2015, Indian Journal of Endocrinology and Metabolism). This was another knob we could turn.
The conclusion we shared with her was calm and specific: “Your body is not broken. Your body is overwhelmed. Let’s unwind it, in order.”
The Plan
We did not put Gowri on an aggressive diet. We did not give her a long list of supplements. The last thing she needed was another extreme intervention.
The plan was the opposite. Simple. Consistent. Sustainable.
Nutrition: Balanced Indian Meals, Designed Around Her
Our nutritionist team built her a personalised nutrition plan centred on familiar Indian foods, not exotic imports.
The focus was:
- Balanced plates: protein, complex carbohydrates, vegetables, and healthy fats at every meal
- Consistent meal timing: eating at similar times every day to stabilise insulin
- Normal Indian kitchen foods: dal, brown rice, ragi, vegetables, curd, eggs, paneer, fish; not superfoods she’d have to hunt for
- Portions tailored to her body, not a generic chart
- Nourishment, not deprivation: the opposite of the crash diets she had tried before
Gowri would sometimes send photos of her plates. The team would give small feedback, not rewrites, small nudges: “Add a little more protein here. This looks great.”




(For the broader framework, see our fertility diet for women and how to eat for PCOS guides.)
Movement: Consistent, Not Extreme
We did not prescribe intense workouts. At 95 kg with uncontrolled sugar, the priority was building a movement habit her body could sustain, not punishing it.
- Daily walking, gradually increasing
- Simple bodyweight exercises tailored to her energy and joints
- No “burn” days or extreme sessions. Consistency over intensity.
- Rest days built in, explicitly allowed
The goal was simple: move every day. Don’t break the chain.
(See our guide on PCOS exercise: what actually helps for the same philosophy in more detail.)
Sleep, Stress, and the Emotional Layer
Women with long-standing PCOS and fertility struggles carry more than metabolic stress. Gowri carried the exhaustion of having tried and failed, the comments of family, the quiet fear that her body had let her down.
For more on this, read our guide on Stress & PCOS. So the programme also included:
- Weekly reviews with the nutritionist team
- Monthly reviews with Dr. Suganya
- Daily check-ins and daily accountability
- Stress-management inputs: phone/social-media boundaries, sleep routine, how to respond to negative comments from relatives
- Permission to feel proud of small wins
Thyroid Optimisation
We asked her to retest thyroid in a few weeks and coordinated with her doctor on adjustments. The goal was to get her TSH well below 2.5 µIU/mL before she conceived.
The Journey
Month 1: Her Body Started Listening
Within the first few weeks, Gowri’s energy shifted. She was lighter. She was sleeping better. She was cooking for herself. And then, something she had almost stopped expecting, her periods came on their own, without withdrawal pills.
For someone who had needed tablets to bring on cycles for years, this was a quiet earthquake.
Month 2: The Skin and the Scale
By Month 2, two things were visibly different:
- Her acanthosis nigricans (that darkened velvety skin at the neck and underarms) had started to fade, a visible sign her insulin sensitivity was improving
- Her weight was steadily dropping, not in crash mode, but consistently
She wasn’t obsessing over the scale. She was simply following the plan. The plan was doing the work.
Month 3: The Numbers Caught Up
At around the 2.5 to 3-month mark, we retested her labs. The difference was significant.
And her weight:
In her own words to our team:
“I am very happy to share the few points. When I have started this program my total life has been changed. I was very happy and energetic. I have to thank all.”
A short message. But read it again. “My total life has been changed.”
Her Full Reflection
Later, she sent us a longer message summarising her experience.
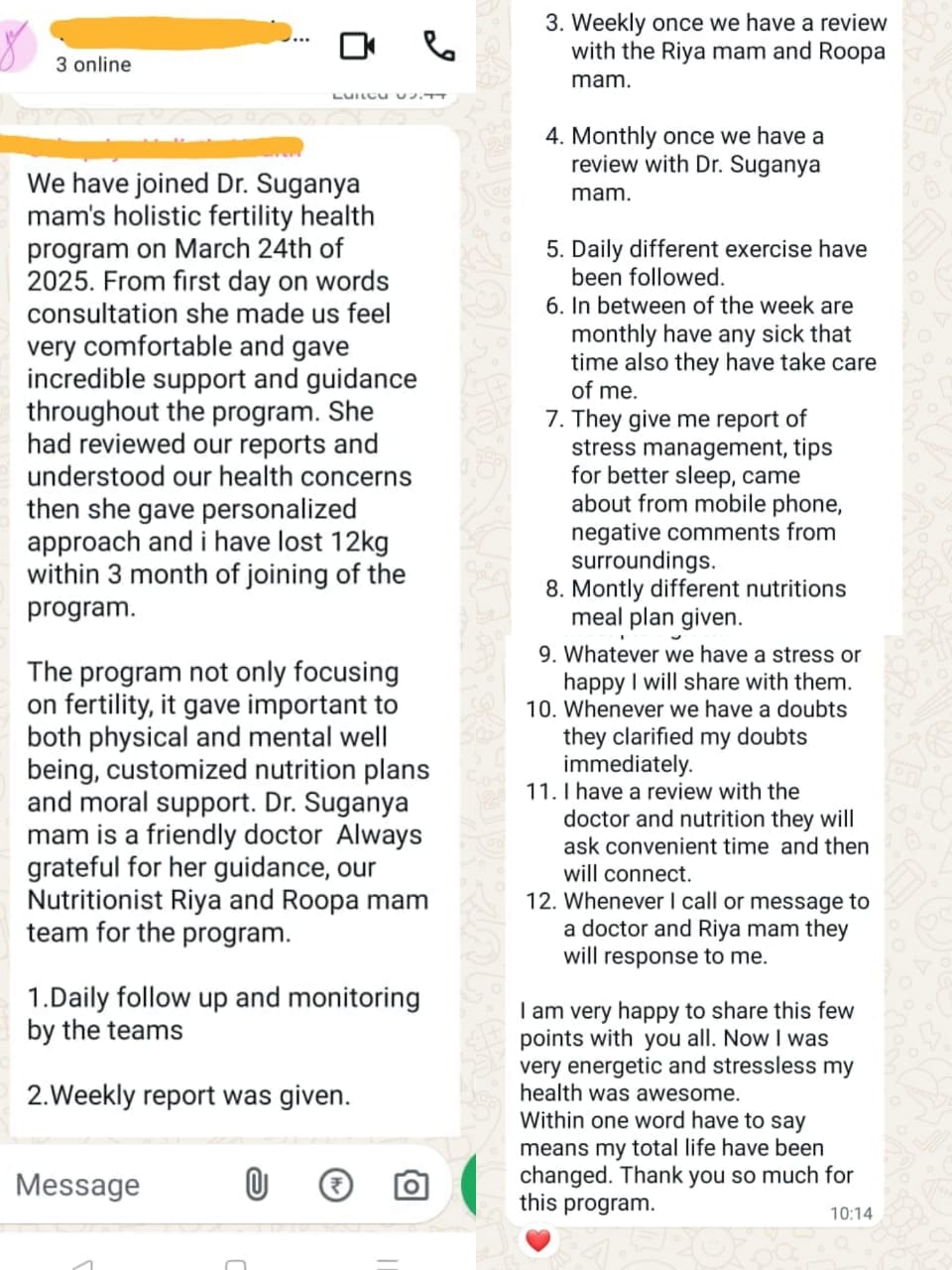
Her own words (verbatim, lightly formatted):
“We have joined Dr. Suganya mam’s holistic fertility health program on March 24th. From first day onwards consultation she made us feel very comfortable and gave incredible support and guidance throughout the program. She had reviewed our reports and understood our health concerns, then she gave a personalized approach and I have lost 12 kg within 3 months of joining the program.
The program not only focusing on fertility, it gave importance to both physical and mental well being, customized nutrition plans and moral support. Dr. Suganya mam is a friendly doctor. Always grateful for her guidance and our nutritionist team for the program.
Daily follow up and monitoring by the teams. Weekly reports were given. Weekly reviews with the nutritionist team. Monthly review with Dr. Suganya mam. Daily different exercises. Whenever I was sick they took care of me. They gave me reports on stress management, tips for better sleep, guidance on phone use, and how to handle negative comments from surroundings. Monthly different nutrition meal plans. Whenever I had stress or happiness I shared with them. Whenever I had doubts they clarified immediately.
I am very happy to share these points with you all. Now I am very energetic and stress-less, my health was awesome. Within one word I have to say, my total life has been changed. Thank you so much for this program.”
Back to Her Doctor: And Then It Worked
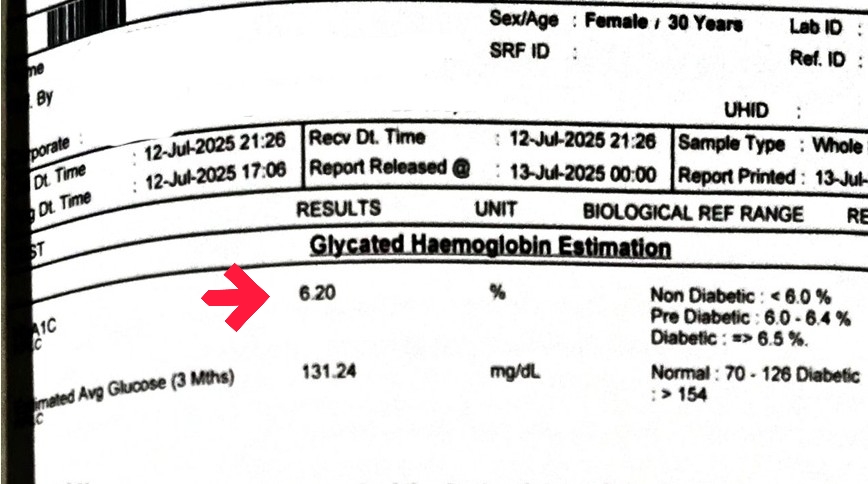
Once Gowri’s parameters were where they needed to be (HbA1c 6.2%, TSH 2.65, weight 81 kg, natural cycles restored), we did exactly what was planned from day one.
We sent her back to her gynaecologist.
Her doctor reviewed the new reports. The next cycle, she started ovulation induction.
In that one cycle, Gowri conceived.
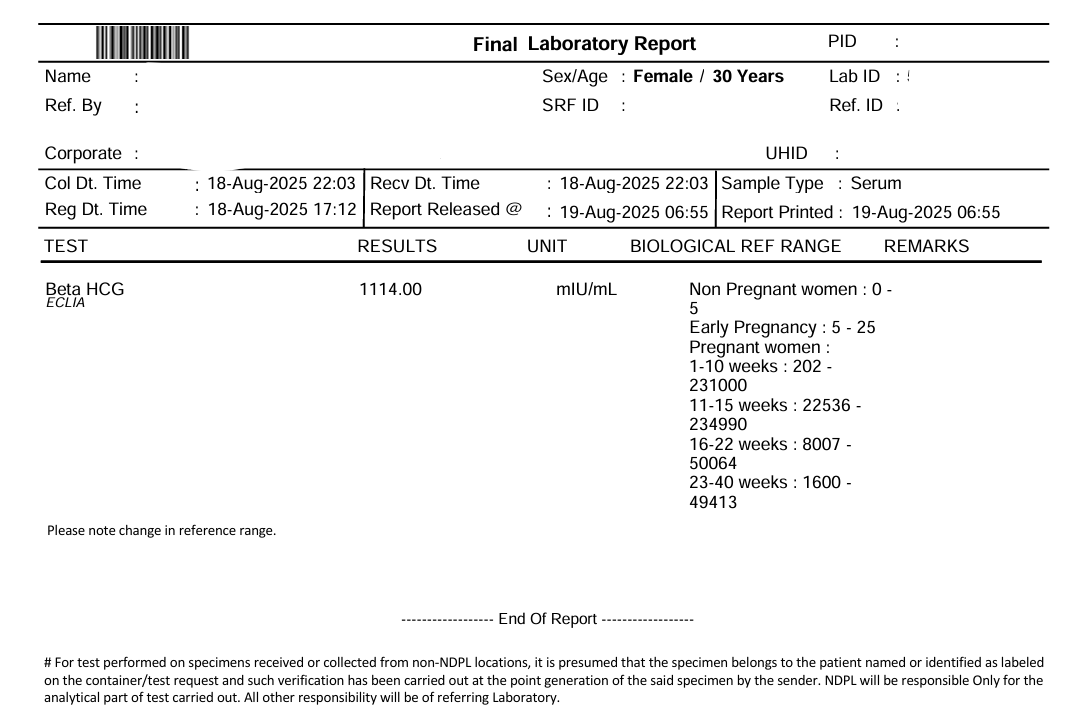
The beta HCG of 1114 mIU/mL placed her in the early-pregnancy range. After a long struggle, after severe metabolic dysfunction, after “nothing is working”; one cycle of ovulation induction worked, because her body was finally ready.
The Outcome
| Metric | Before (March) | After (July) |
|---|---|---|
| Weight | 95 kg | 81 kg (−14 kg) |
| BMI | 38.1 (obesity) | 32.4 (still overweight, but significantly lower risk) |
| HbA1c | 9.8% (diabetic range) | 6.2% (near-normal) |
| Avg glucose | 234 mg/dL | 131 mg/dL |
| TSH | 3.21 µIU/mL | 2.65 µIU/mL (preconception-preferred) |
| Periods | Needing withdrawal pills | Spontaneous, natural cycles |
| Acanthosis nigricans | Clinically present | Fading |
| Fertility outcome | Years of TTC, unable to start treatment safely | Conceived in 1 cycle of ovulation induction |
Severe metabolic dysfunction, reversed in 3 months. One ovulation induction cycle. Pregnancy confirmed.
💜 If You’ve Been Told Your Body Isn’t Ready Yet
High HbA1c, high BMI, irregular cycles, or PCOS flagged before fertility treatment are not a door closing. They’re a window to prepare. The women who use that window well often need less medical intervention later, not more.
🩺 Why Doctors Are Referring Their Patients to Us Before Starting Fertility Treatment
A note for gynaecologists and fertility specialists, from Dr. Suganya.
If you are a treating gynaecologist reading this, the reason Gowri’s story matters is not just that she conceived. It’s that she conceived more easily than she would have without preparation, with lower risk to the pregnancy, and with less medication than would have been needed had she entered treatment at 95 kg and HbA1c 9.8%.
This is not anecdote. The evidence base is real and growing.
1. BMI and ART outcomes. A 2024 systematic review and meta-analysis in Scientific Reports (Park et al.) examining weight loss before IVF in women with obesity and infertility found improved pregnancy outcomes in the weight-loss groups, and recommended preconception weight loss as a reasonable component of fertility planning. A 2025 pilot study (Espinós et al., Reproductive BioMedicine Online) reported a cumulative live birth rate of 61.9% in a 12-week diet-and-exercise-intervention group vs 30% in controls undergoing IVF.
2. Lifestyle intervention before infertility treatment. The Dutch LIFEstyle trial (Mutsaerts et al., NEJM 2016) randomised obese infertile women to a 6-month preconception lifestyle intervention versus immediate fertility treatment. Follow-up analyses (PLOS One, 2018; IJBNPA, 2018) showed improvements in diet, physical activity, cardiometabolic health, and natural conception rates in the intervention arm. The FIT-PLESE trial (Legro and colleagues, PLOS Medicine, 2022) similarly demonstrated improved ovulation and pregnancy outcomes after a structured preconception programme in obese women with unexplained infertility.
3. Glycaemic control before pregnancy. For women with diabetes or prediabetes, every major guideline recommends an HbA1c target of <6.5% (ideally <6.0%) before conception. Higher preconception HbA1c is independently associated with miscarriage, congenital anomalies, and perinatal complications (Xodo et al., Medicina, 2021; Journal of Clinical Endocrinology & Metabolism, 2022). Starting ovulation induction or IVF at HbA1c 9.8% is clinically unsafe; preparing first is not “delay,” it is standard of care.
4. PCOS-specific evidence. The 2023 International Evidence-Based PCOS Guideline (Teede et al.) reaffirms lifestyle modification as first-line treatment for overweight and obese women with PCOS, particularly before ART. The Thessaloniki consensus similarly positions lifestyle before medical induction.
What Fertilia adds when you refer a patient to us:
- A 90-day structured programme with daily nutritionist follow-up, monthly OB-GYN review (Dr. Suganya), and a clear handoff back to you with updated reports
- No disruption to your clinical plan, we do not prescribe fertility medication or perform procedures; we optimise the metabolic and hormonal environment you will be treating
- Explicit measurement: HbA1c, TSH, weight, cycle regularity, insulin markers where relevant
- Patient adherence support: the hardest part of lifestyle change is consistency; our daily touchpoints are how that gets delivered
When referring makes most sense: BMI >30 with insulin-resistant PCOS, HbA1c >6.5%, uncontrolled thyroid, or a failed prior ART cycle where metabolic factors were likely contributors.
If you’d like to discuss a patient or understand how we fit alongside your clinical plan, Dr. Suganya is personally available at +91 99402 70499. There is no commercial referral relationship; patients remain under your care throughout.
What This Story Teaches Us
1. Preparation is not a delay. It is part of the treatment.
Gowri “lost” three months to preparation. What she gained was a pregnancy in the very next cycle, on the simplest medical intervention (ovulation induction, no IUI, no IVF), with significantly lower pregnancy risk. That is an extraordinarily efficient use of three months.
2. A BMI of 38 and HbA1c of 9.8 are reversible. Faster than most people think.
There is a persistent myth that severe metabolic dysfunction takes years to fix. It does not. With structured nutrition, consistent movement, and accountability, HbA1c can drop 2–3 percentage points in three months. Weight can move 10–15 kg. Periods can return within weeks. Gowri is not an outlier. She is what’s possible when the plan matches the body.
3. Doctors working with doctors is good medicine.
Gowri’s gynaecologist did not hand her off. She looped us in, received the updated reports, and then resumed treatment. That is the model we believe in: the gynaecologist handles the medical side, we add the lifestyle foundation, and the patient wins from both. (Related case study: How Nisha Reversed Her PCOS and Got Pregnant)
4. The absence of extreme dieting is the point.
Gowri had tried multiple diets. None had stuck. The Fertilia plan worked precisely because it wasn’t another crash. Sustainable metabolic change needs a sustainable plan. Anything else is going to fail the moment life gets in the way. (Also see: PCOS Belly: Why It Happens and How to Reduce It)
5. A good ending is often a handoff, not a finale.
Our programme ended when Gowri went back to her doctor. Her story continued there. That’s how these stories are supposed to end: with the patient returning to her primary care team stronger, more informed, and more biologically ready.
Frequently Asked Questions
Why does HbA1c need to be below 6.5% before pregnancy?
Uncontrolled blood sugar in early pregnancy increases the risk of miscarriage, congenital anomalies (particularly cardiac and neural tube defects), and gestational diabetes. The developing embryo is most sensitive in the first 6–8 weeks, often before a woman even knows she’s pregnant, which is why the target is to normalise HbA1c before conception, not during the first trimester (Xodo et al., 2021, Medicina; international preconception diabetes guidelines). For women with PCOS who also have insulin resistance, the same principles apply.
Is 3 months really enough to reverse an HbA1c of 9.8%?
HbA1c reflects your average blood sugar over roughly the previous 3 months. It responds to consistent changes in blood sugar over that window. With a structured nutrition plan, consistent movement, and daily accountability, a drop of 2–4 percentage points in 3 months is clinically realistic, as Gowri’s case demonstrates (9.8% → 6.2%). The key word is “consistent.” Without structure, the same intention rarely produces the same result.
If my doctor says I need to lose weight before fertility treatment, am I being delayed?
No. You’re being prepared. The studies above (FIT-PLESE, LIFEstyle, Espinós 2025) show that preconception lifestyle interventions can nearly double live birth rates in women with obesity and infertility. A good gynaecologist who asks you to prepare before ART is thinking long-term about your pregnancy outcomes, not short-term about the cycle. The three months Gowri spent preparing collapsed her treatment timeline dramatically. She conceived in the very next cycle.
Does Fertilia prescribe fertility medication?
No. Our role is lifestyle, nutrition, metabolic, and hormonal optimisation. Fertility medication, procedures (IUI, IVF, ovulation induction), and clinical management stay with your treating gynaecologist. We send you back to them with updated reports. Many of our patients, like Gowri, conceive with minimal medical intervention because their bodies are finally ready to respond.
I don’t have a referring doctor. Can I still join?
Yes. Many women come to us directly. If fertility treatment turns out to be the right next step for you, Dr. Suganya will say so clearly and help you find the right gynaecologist or fertility specialist. Our goal is your outcome, not retaining you in our programme.
What’s different about Fertilia’s approach compared to a diet plan or a gym membership?
Three things. First, it’s personalised: the plan is built around your reports, your starting point, and your body, not a generic template. Second, it’s integrated: one medical doctor (OB-GYN), one nutritionist team, one coordinator, all seeing the same picture. Third, it’s supported daily: the difference between information and transformation is accountability. A PDF plan and a standalone gym membership cannot do what daily team contact can. That’s the single biggest reason women who’ve “tried everything” finally see results with us.
This is part of our ongoing series of real patient case studies. Every story is verified and shared with the patient’s consent. Names and identifying details are changed to protect privacy.
Dr. Suganya Venkat is an OB-GYN with 15+ years of clinical experience. She holds a DNB in OB-GYN from GKNM Hospital (Coimbatore), an MD in Pathology from CMC Vellore, and an MBBS with 5 Gold Medals from SRMC.



