

Name has been changed to protect patient privacy. Clinical details and images are shared with the patient’s consent.
Yamuna understood medicine better than most of our patients.
She was a 26-year-old MBBS graduate, preparing for her postgraduation entrance examination. She had studied the human body for years. She knew what PCOS was, what hormones did, and how cycles were supposed to work.
But knowing and healing are two very different things.
Her periods came once every 2 to 3 months, and even that was usually after taking a tablet. Her scan showed polycystic ovaries. Her prolactin levels were in the 60s (normal is roughly 2 to 29 ng/mL), clearly pointing towards a deeper hormonal disruption.
On paper, she didn’t look like someone who was struggling. She was lean: 168 cm, 57 kg. No weight problem. No visible red flags.
But underneath, everything was unravelling.
What Was Really Going On
When we first started working with Yamuna, she appeared calm and composed. She understood the science. She nodded along with the plan.
But as the conversations deepened, a very different picture emerged.
This was not just PCOS. This was stress taking over her body.
Multiple layers of it, all building up at the same time:
- Exam pressure: postgraduation entrance preparation is one of the most intense experiences in Indian medicine
- Recent marriage: the emotional adjustment of building a new life
- Husband working at sea: sudden long-distance, limited contact
- Lack of a support system: no one to talk to about what she was going through
Stress doesn’t just affect your mood. Chronic psychological stress directly disrupts the hypothalamic-pituitary-ovarian axis, the hormonal communication pathway that governs ovulation. When cortisol stays elevated, the body deprioritises reproduction (Chrousos, 1998, NEJM). Elevated prolactin, like Yamuna’s, is a well-documented consequence of chronic stress and can independently suppress ovulation (Lennartsson & Jonsdottir, 2011, Psychoneuroendocrinology).
Her body wasn’t “broken.” It was overwhelmed.
When Everything Started Slipping
As the stress accumulated, Yamuna’s routine began to collapse. Not because she didn’t know what to do. She was a doctor. She knew exactly what a healthy routine looked like.
But she didn’t have the mental space to follow one.
The meals went first:
- No breakfast
- No lunch
- Dinner irregular, sometimes skipped entirely
Then came a cascade of physical symptoms:
- Gastritis: constant stomach irritation
- IBS-like symptoms: gut disturbance that made eating uncomfortable
- Poor sleep: lying awake with a racing mind
- Sleeping pill dependence: the only way she could get rest
At this point, the case had become something much larger than PCOS. It was:
- Hormonal imbalance
- Gut disturbance
- Emotional overload
- Complete lifestyle breakdown
Each one was feeding the others. The stress worsened the gut. The gut issues made eating miserable. Not eating disrupted her hormones. The hormonal disruption worsened her mood and sleep. And around it went.
Where We Actually Started
Here is where Yamuna’s story diverges from most case studies you’ll read.
We didn’t start with a diet plan. We didn’t start with an exercise routine. We didn’t even start with supplements.
We started with a conversation.
That one call lasted more than 1.5 hours.
Yamuna cried. She spoke openly about things she hadn’t told anyone: the loneliness, the pressure, the feeling that her body was failing her despite all her medical knowledge.
And honestly, that conversation was the real starting point of her healing. Not the nutrition. Not the movement. Being heard.
Because you can hand someone the most perfectly designed plan in the world. If they don’t have the emotional foundation to follow it, nothing will stick.
📞 Feeling Overwhelmed and Not Sure Where to Start?
If stress, gut issues, or emotional exhaustion are wrapped up in your PCOS, you’re not alone. Dr. Suganya’s programs look at the full picture, not just your ovaries.
One Simple Goal: Eat Three Meals a Day
After that conversation, we designed the simplest possible starting point.
Not a macro-balanced meal plan. Not a calorie target. Not an anti-inflammatory protocol.
Just: eat three meals a day.
That’s it.
Because at that moment:
- Her gut was so sensitive that complex meal plans would have been counterproductive
- Her mind was overwhelmed, and any additional complexity would have felt like more pressure
- Her body needed stability first, not perfection
We didn’t need her to eat perfectly. We needed her to eat consistently.
The First Shift: Sleep
Within 15 days, something important happened.
Yamuna slowly reduced her dependence on sleeping pills. She started sleeping naturally.
For someone who had needed medication just to fall asleep every night, this was a significant change.
The daily check-ins tell the story. Consistent bedtimes. Regular wake-up times. 2 litres of water. Workouts happening. Mood stabilising from “struggling” to “okay.” These small data points, tracked every day, were signs that her nervous system was calming down.
Sleep restoration is not just about feeling rested. It directly influences cortisol regulation, prolactin levels, and the hormonal signalling that drives ovulation (Kloss et al., 2015, Journal of Clinical Sleep Medicine). Fixing Yamuna’s sleep was a prerequisite for fixing everything else.
Healing the Gut
As Yamuna started feeling better mentally, everything else slowly followed.
She started eating regularly. Not perfectly, but consistently. Three meals a day became the norm. And as her eating stabilised, her gut began to calm down.





Look at those plates. Nothing extreme. Nothing complicated. Dosa with eggs and chutney. Rice with dal and poriyal. Toast with egg and paneer. Regular Indian food, balanced across protein, carbs, and fats.
Within a month:
- No sleeping pills
- No gastritis medication
- Better energy
- A more stable daily routine
The gut-hormone connection is well established. Chronic gut inflammation disrupts oestrogen metabolism and can worsen hormonal imbalance in PCOS (Tremellen & Pearce, 2012, Medical Hypotheses). By healing her gut first, we were clearing the way for her hormones to normalise.
Building Back Strength
Yamuna didn’t rush anything. She gradually added:
- Regular, structured meals
- Gentle movement
- Short workouts
Not because we pressured her, but because she was starting to feel better and her body wanted to move.
Her body responded:
- Abdominal fat reduced
- She felt lighter and more energetic
- A sense of control returned
For women with lean PCOS, the goal isn’t weight loss. It’s about body composition, metabolic function, and hormonal balance. Even at a healthy weight, the right nutrition and consistent movement make a measurable difference to how the body processes hormones. (If you want to understand how lean PCOS works differently, our Lean PCOS: How Sujatha Got Her Periods Back case study covers the science in detail.)
A New Challenge: Hostel Food
Around this time, Yamuna cleared her postgraduate entrance examination. A big achievement, and well-deserved.
She joined a hospital. But this brought a new challenge: hostel food.
The hostel meals were too spicy, not suitable for her still-recovering gut.
So we adapted. We didn’t expect her to follow the plan perfectly in a hostel setting. We guided her on:
- Making better choices from what was available
- Simple alternatives she could manage
- Adding protein and vegetables to whatever the hostel served
She’d already built the habits. She knew how to work with constraints, not against them. (This practical, real-world approach to hostel food is something we’ve refined across multiple patients. If you’re a student dealing with PCOS, our PCOS Diet Chart has hostel-friendly tips.)
The Moment: Natural Periods
And then came the shift that changed everything.
Yamuna got her period. Naturally. No tablets.
For someone who had depended on medication for every single cycle, this was deeply reassuring. Her body, given the right environment, was finally doing what it was supposed to do on its own.
The next month? It came again. On time. A proper 28-day cycle.
“Without even taking any medications for this cycle I got my periods naturally. I’m so happy about it. I want to thank mam, Elakiya and your team for guiding me and motivating me to do it.”
That message captures something statistics never can. The relief. The gratitude. The quiet amazement that her body could do this on its own, after all those years of tablets and doubt.
And Then…
After the program ended, Yamuna’s life continued to stabilise. Her husband returned. Her routine held. She continued the habits she had built.
And then, a few months later, the news arrived.
She was pregnant. Naturally. Without any fertility treatment.
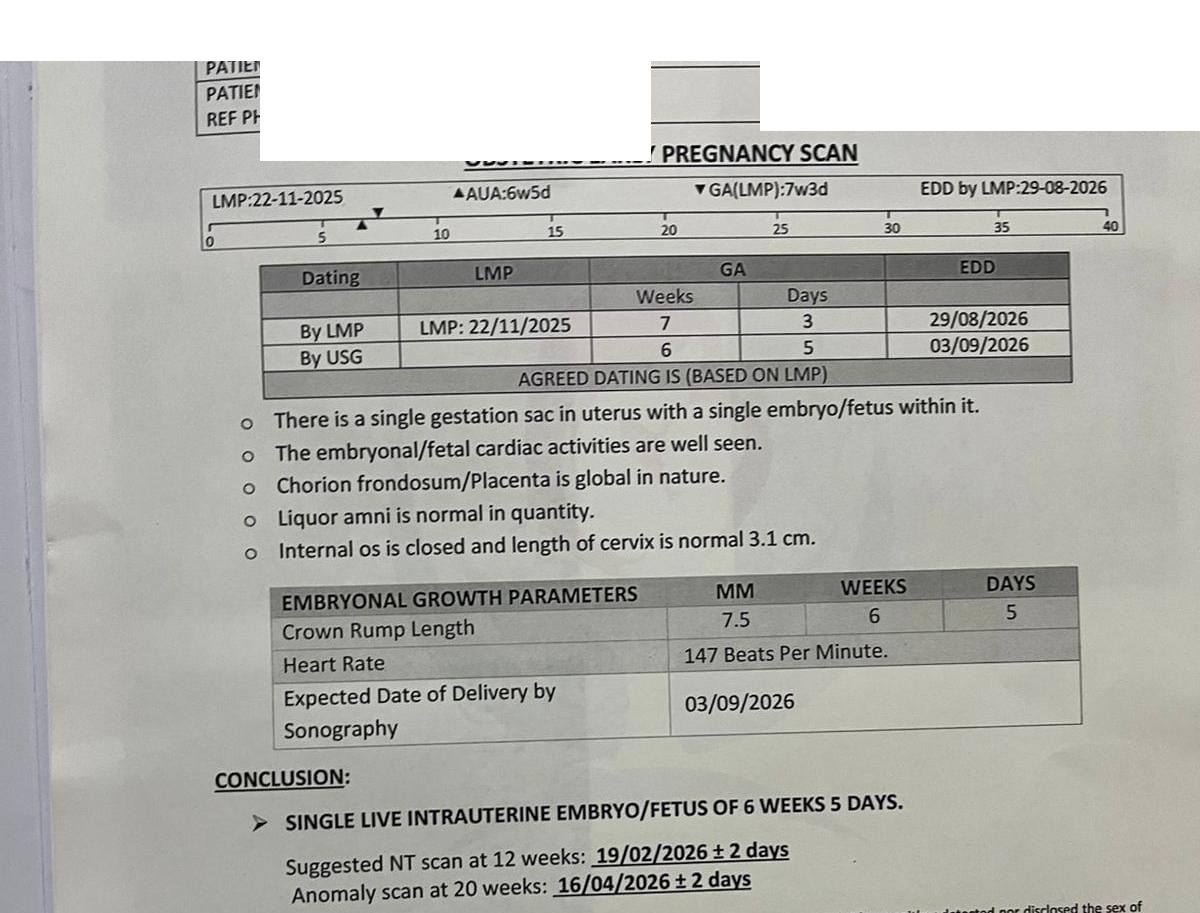
Her scan confirmed a healthy pregnancy: single live intrauterine embryo, normal cardiac activity, everything progressing exactly as it should.
This is the same woman who had been dependent on tablets just to get a period. Whose body was so stressed that her prolactin had climbed to twice the normal level. Who was surviving on sleeping pills and skipping meals.
Natural conception. No IVF. No IUI. No ovulation induction. (For women still in the pre-conception stage, our guide to getting pregnant naturally covers the evidence-based steps.)
What Dr. Suganya Observed
This is what makes Yamuna’s case particularly meaningful:
“Yamuna is now so happy and confident about the effect of lifestyle modification. She got pregnant naturally when she had no hope of getting pregnant naturally. She has vowed that she will make sure all her patients are explained about the importance of lifestyle modifications to improve their hormonal and metabolic health.”
A doctor who became a patient. Who experienced, firsthand, that healing isn’t just about knowing the science. And who now carries that understanding into her own clinical practice.
That might be the most lasting outcome of this entire case.
What This Case Study Teaches Us
1. Stress is a real, measurable PCOS driver
Stress is not “all in your head.” Chronic psychological stress elevates cortisol, disrupts the HPO axis, raises prolactin, suppresses ovulation, and worsens gut permeability. Yamuna’s elevated prolactin in the 60s (roughly double normal) was a direct biochemical marker of what stress was doing to her body. When the stress was addressed, the prolactin came down and her cycles returned, and if you want to know what to look for when ovulation resumes, our guide on ovulation symptoms explains every physical sign the body gives.
2. Medical knowledge alone doesn’t protect you
Yamuna was a doctor. She understood hormones, cycles, and PCOS better than most people. But understanding a condition intellectually and having the emotional support and structured guidance to heal from it are completely different things. This is why personalised, supported programmes exist. Knowing what to do is not the same as having the capacity to do it consistently, especially under stress.
3. Sometimes the first step is emotional, not physical
Most health programmes start with a diet plan or exercise routine. Yamuna needed something different first: to be heard. That 1.5-hour conversation, where she could finally express what she was going through, created the emotional foundation for everything that followed. Without it, any plan we gave her would have become just another thing she “should” be doing but couldn’t.
4. The gut and the hormones are deeply connected
Yamuna’s case illustrates the gut-hormone axis beautifully. Stress destroyed her gut health (gastritis, IBS). The gut inflammation worsened her hormonal imbalance. Healing the gut through consistent, simple meals was a prerequisite for hormonal recovery. You can read more about how insulin resistance and PCOS interact with metabolic health, and how PCOS belly fat is often driven by the same inflammatory pathway.
5. Start simple. Build gradually.
“Eat three meals a day” sounds almost too basic to be a medical intervention. But for someone whose entire routine had collapsed, that simplicity was exactly right. Complexity would have added more stress. Simplicity gave her something achievable, something she could succeed at on Day 1. The more complex interventions came later, after the foundation was solid.
💜 Is Stress Wrapped Up in Your PCOS?
Every woman’s PCOS has different drivers. For some, it’s insulin resistance. For others, it’s inflammation. For Yamuna, it was stress. A thorough assessment can help identify what’s actually driving your symptoms, so the plan addresses the root cause, not just the surface.
Frequently Asked Questions
Can stress alone cause PCOS or irregular periods?
Stress can be a significant driver of menstrual irregularity, and in some cases it can mimic or worsen PCOS. Yamuna’s diagnosis was confirmed through ultrasound (polycystic ovaries) and clinical hormone workup, meeting the Rotterdam Criteria. Chronic stress elevates cortisol, which disrupts GnRH pulsatility (the signal that tells your ovaries to ovulate). It can also raise prolactin levels, which independently suppresses ovulation. In Yamuna’s case, stress was the dominant factor. Her lean body type and elevated prolactin both pointed to a stress-driven hormonal pattern rather than the insulin-resistant pattern more commonly associated with PCOS.
What does elevated prolactin mean for fertility?
Prolactin is a hormone that normally rises during breastfeeding to suppress ovulation (this is nature’s way of spacing pregnancies). When prolactin is elevated outside of breastfeeding, it can suppress the hormonal signals needed for regular ovulation and menstrual cycles. Mild to moderate elevations (like Yamuna’s levels in the 60s) can be caused by chronic stress, certain medications, or a small pituitary adenoma. The cause needs proper investigation, but when stress is the driver, addressing the stress can bring prolactin down naturally.
Can lifestyle changes help if my PCOS is stress-driven?
Yes. Stress-driven hormonal disruption is one of the most responsive patterns to lifestyle intervention. The key interventions are: stress management (emotional support, breathing practices, consistent sleep), gut healing (regular meals, anti-inflammatory foods), and gradual movement. In Yamuna’s case, these changes restored her cycles within a few months and she conceived naturally without any fertility medication.
Why did you start with emotional support instead of a diet plan?
Because Yamuna’s primary barrier was not nutritional ignorance. She was a doctor. She knew exactly what a healthy meal looked like. Her barrier was emotional overwhelm, chronic stress that had left her unable to follow any plan at all. Starting with emotional support (that 1.5-hour call, being heard without judgement) created the psychological safety she needed before anything else could work. This is something we assess individually for every patient.
Is lean PCOS the same as regular PCOS?
PCOS is one syndrome with multiple drivers. In lean PCOS, the external markers (weight, BMI) look normal, but the hormonal and metabolic disruption is very much present. The drivers in lean PCOS tend to be inflammation, adrenal androgen excess, nutritional deficiencies, or stress, rather than insulin resistance alone. Lean PCOS requires the same structured, personalised approach, but the interventions are different. Our guide on PCOS: Symptoms, Root Causes & Treatment covers all the recognised drivers.
How long did it take for Yamuna’s cycles to come back?
Yamuna’s natural periods returned during the program itself. The first natural period (without tablets) came after consistent lifestyle changes over the initial weeks. The following month, she had a regular 28-day cycle. She continued to have natural periods even after the program ended, and conceived naturally a few months later.
How is Fertilia’s approach different from just telling someone to “reduce stress”?
“Reduce stress” is advice. It’s not a plan. At Fertilia, we identify the specific ways stress is manifesting in your body (through hormone panels, gut assessment, sleep and routine analysis) and then build a step-by-step programme to address each layer. For Yamuna, that meant: emotional support first, then sleep restoration, then gut healing through consistent meals, then gradual movement and strength building. Each step was sequenced deliberately based on what her body needed at that stage, not what a generic wellness plan would prescribe.
This is the fifth in our series of patient case studies from our clinic. Every story is real, verified, and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.
Dr. Suganya Venkat is an OB-GYN with 15+ years of experience. She holds an MBBS (SRMC, 5 Gold Medals), MD in Pathology (CMC Vellore), and DNB in OB-GYN (GKNM Hospital, Coimbatore).



