

Names have been changed to protect patient privacy. Clinical details are shared with the couple’s consent.
Lalitha and Vivek came to us in their early thirties, ready to move forward with IVF. Emotionally, the decision had already been made. The discussions with their fertility specialist had happened. The next cycle was on the calendar.
But their bodies were not yet ready to support what they were about to ask of them.
Lalitha, 33, was carrying years of PCOS, painful and irregular cycles, heavy bleeding, a BMI of 50.5 (Class III obesity, the range often described as morbid obesity), hypothyroidism, elevated blood pressure, and the quiet exhaustion of having been told more than once that her egg reserve was low. She had already been through two follicular studies with inconsistent results.
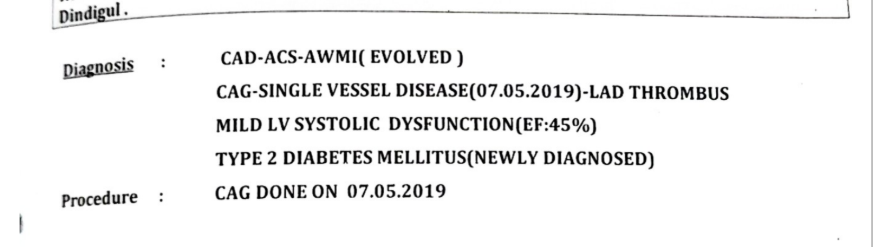
Vivek, 36, was carrying a different kind of weight. In 2019, in his late 20s, he had experienced chest pain and undergone an angiogram that revealed a single vessel blockage in his LAD with a thrombus, a mildly reduced ejection fraction, and newly diagnosed Type 2 diabetes. He had been on Acitrom for three months after that event. Six years later, his diabetes was still uncontrolled, his thyroid was elevated, and his central obesity had crept back.
This was not a single problem to solve. It was a combination of metabolic, hormonal, and cardiovascular realities, in both partners, sitting right in front of what should have been a hopeful next step.
They did not want to walk into IVF with their bodies in this state. They wanted to prepare.
The Starting Point
When Lalitha and Vivek joined the program, we spent the first consultations not talking about IVF at all. We talked about what was happening inside their bodies and why it mattered before any transfer.
Lalitha’s profile
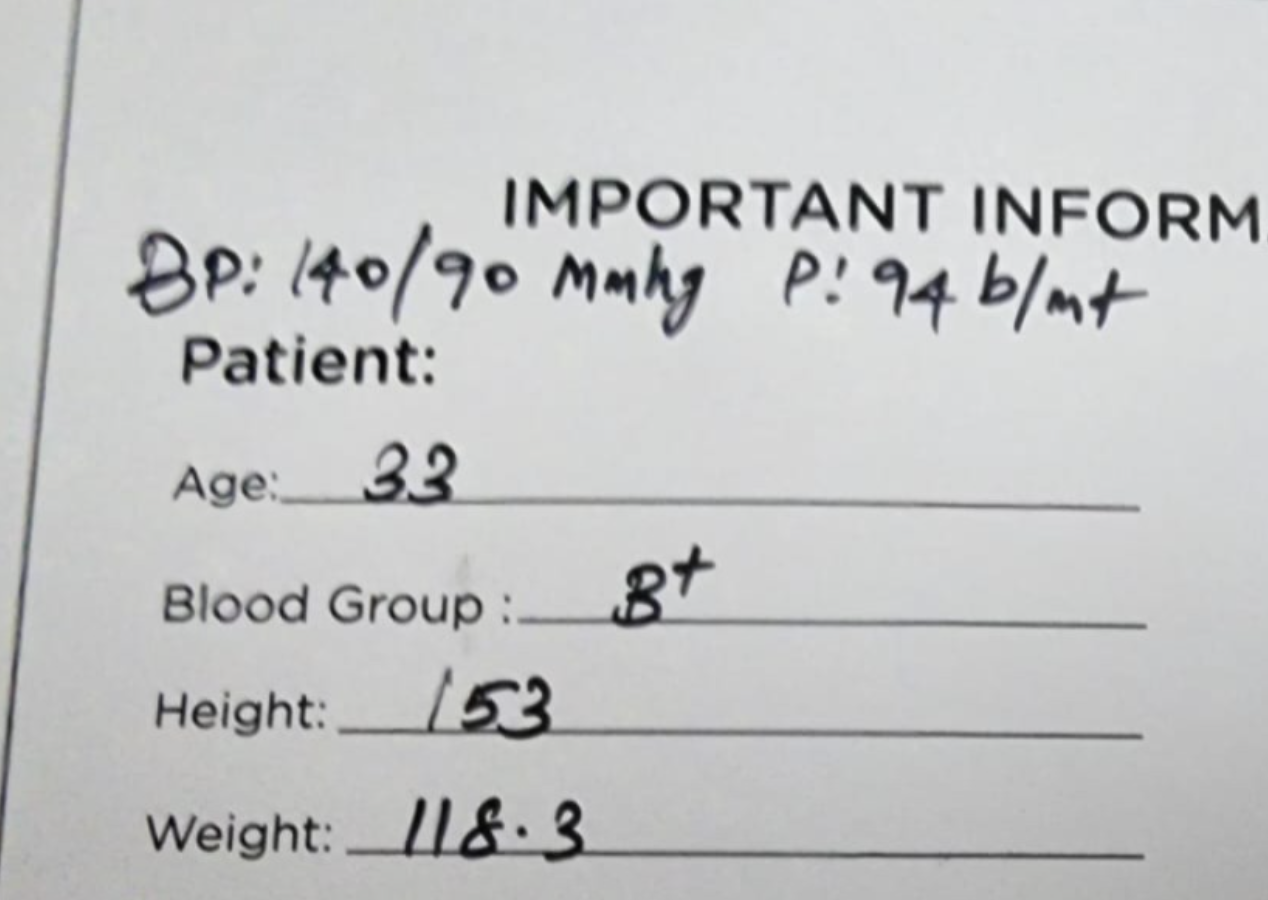
- Age: 33
- Height: 153 cm
- Weight: 118.3 kg (BMI 50.5, Class III obesity)
- BP: 140/90 mmHg, pulse 94 bpm
- Conditions: PCOS, hypothyroidism, irregular cycles with heavy bleeding, hirsutism, hair thinning
- Follicular studies: 2 prior, with inconsistent hormonal rhythm
- Fertility history: Told her egg reserve was low
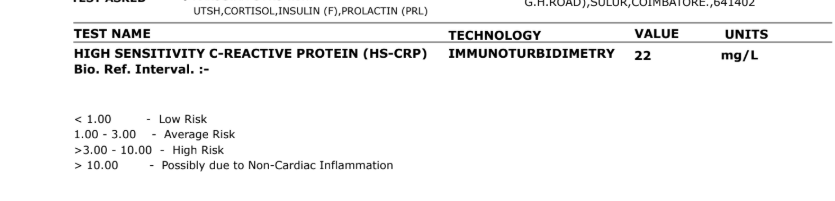
Her TSH at entry was 4.24 µIU/mL (on the upper side of the reference range), her hs-CRP was 22 mg/L (in the “possibly non-cardiac inflammation” range, well above the high-risk threshold of 3 mg/L), and her Vitamin D was 11.2 ng/mL (deficient; sufficiency is 30+ ng/mL).


Vivek’s profile
- Age: 36
- Height: 171 cm
- Weight: 109 kg (BMI 37.3, Class II obesity)
- HbA1c: 6.8% (above the 6.5% diabetic threshold, above the good-control target for a known diabetic)
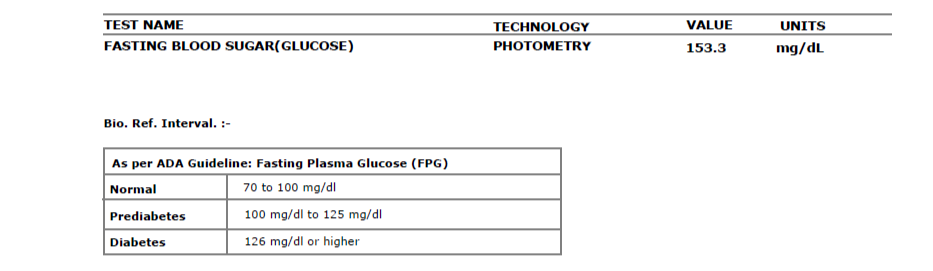
- Fasting glucose: 153.3 mg/dL (diabetic range, over 126)
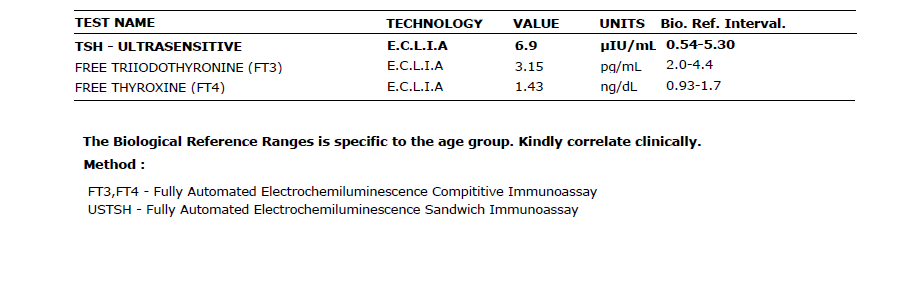
- TSH: 6.9 µIU/mL (elevated; reference upper limit 5.30)
- hs-CRP: 5.29 mg/L (high risk, reference under 3)
- 2019 cardiac event: CAD-ACS with evolved anterior wall MI, single vessel disease with LAD thrombus, mildly reduced ejection fraction (45%), with newly diagnosed Type 2 diabetes at the time
- Medications at joining: Ongoing post-cardiac care, including a history of Acitrom


Both partners were sitting in a high metabolic and inflammatory state. And beyond the numbers were the years. The weight-related comments. The repeated cycle irregularity that made every follicular study feel like waiting to be disappointed. The startup pressure and long hours that kept Vivek from ever quite getting his diabetes under control. The trial-and-error dieting that had never stuck.
They were not careless people. They were stretched thin between responsibility and hope.
Are You Both Preparing for IVF?
If both partners need to optimise their health before a fertility treatment, we can help you build a plan that accounts for PCOS, diabetes, cardiac history, and anything else you are carrying.
Why Both Partners’ Metabolic Health Matters
There is a quiet pattern we see often. Fertility preparation, in most conversations, ends up being about the woman. Her weight. Her cycles. Her ovarian reserve. The male partner’s health gets checked (semen analysis, hormone panel) and, unless something is flagged, often left there.
But IVF outcomes are a two-body story.
1. Insulin resistance affects egg and sperm quality. In women, chronic hyperinsulinaemia drives ovarian androgen production and disrupts follicular development. This is the core mechanism behind PCOS-related ovulatory dysfunction (Dunaif, 1997, Endocrine Reviews). In men, insulin resistance and Type 2 diabetes are associated with lower sperm motility, higher DNA fragmentation, and reduced fertilisation potential (Martins, Majzoub & Agarwal, 2019, World Journal of Men’s Health).
2. Weight affects IVF outcomes in both partners. A BMI over 30 in women is linked to lower live birth rates in IVF (Rittenberg et al., 2011, Reproductive BioMedicine Online). Paternal obesity is separately associated with poorer embryo quality and lower blastocyst rates (Campbell et al., 2015, Reproductive BioMedicine Online). When both partners carry a high BMI, the effects stack.
3. Inflammation quietly lowers implantation. Elevated hs-CRP reflects a systemic inflammatory state that can affect endometrial receptivity and sperm parameters alike. Lalitha’s CRP of 22 and Vivek’s of 5.29 were not separate numbers. They were two parts of the same picture.
4. Thyroid matters for every part of the cycle. Subclinical hypothyroidism (TSH over 2.5 in women trying to conceive) is linked to lower implantation and higher miscarriage rates, and correcting it is considered standard pre-IVF practice (Velkeniers et al., 2013, Human Reproduction Update). Vivek’s elevated TSH also matters; thyroid hormone regulates sperm production and testicular function. We have written more on this in our guide to thyroid and fertility.
Lalitha and Vivek had something in almost every one of these columns. Preparing meant addressing all of it, gently, together.
The Plan
We built the program around what we knew: both partners had serious metabolic concerns, Vivek had a cardiac history that ruled out aggressive exercise, and they had roughly six months before they wanted to move forward with IVF. The plan had to be safe, sustainable, and liveable inside a real marriage with real working hours.
We did not give them a crash diet. We did not put Vivek on intense cardio. We did not promise a fast transformation.
We built a slow, steady, doctor-supervised routine around four pillars.
1. Bloodwork-led supplementation
Before changing anything about food or movement, we reviewed their reports in detail and introduced targeted support where their bodies clearly needed it: Vitamin D for Lalitha’s deficiency, thyroid support calibrated to their TSH trends, and specific nutrients to address the inflammatory markers. Nothing exotic. Nothing that required convincing. Just correcting what the labs were telling us.
2. A portion-controlled, anti-inflammatory Indian plate
Food was where most of their earlier attempts had failed, because most diets ignore what Indian households actually eat. We kept their plates familiar but rebalanced them.
- Complex carbs with a low glycaemic load: ragi, millets, brown rice, whole wheat rotis, portioned properly
- Protein at every meal: dal, paneer, green moong, eggs, dahi, simple non-vegetarian options where they ate them
- Vegetables daily, across the day, for fibre and micronutrients
- Anti-inflammatory building blocks: haldi, jeera, curry leaves, good-quality fats, nothing radical

What made the difference was not novelty. It was that both partners ate the same plate, kept it simple at home, and stayed consistent even on travel days.
That single message tells you more about their journey than any weight graph: even when the day did not go to plan, they stayed in the plan.
3. Walking first, everything else later
Movement had to respect Vivek’s cardiac history. No high-intensity intervals, no unsupervised gym sessions, nothing that would put load on his heart. Walking was the foundation, and it turned out to be enough.
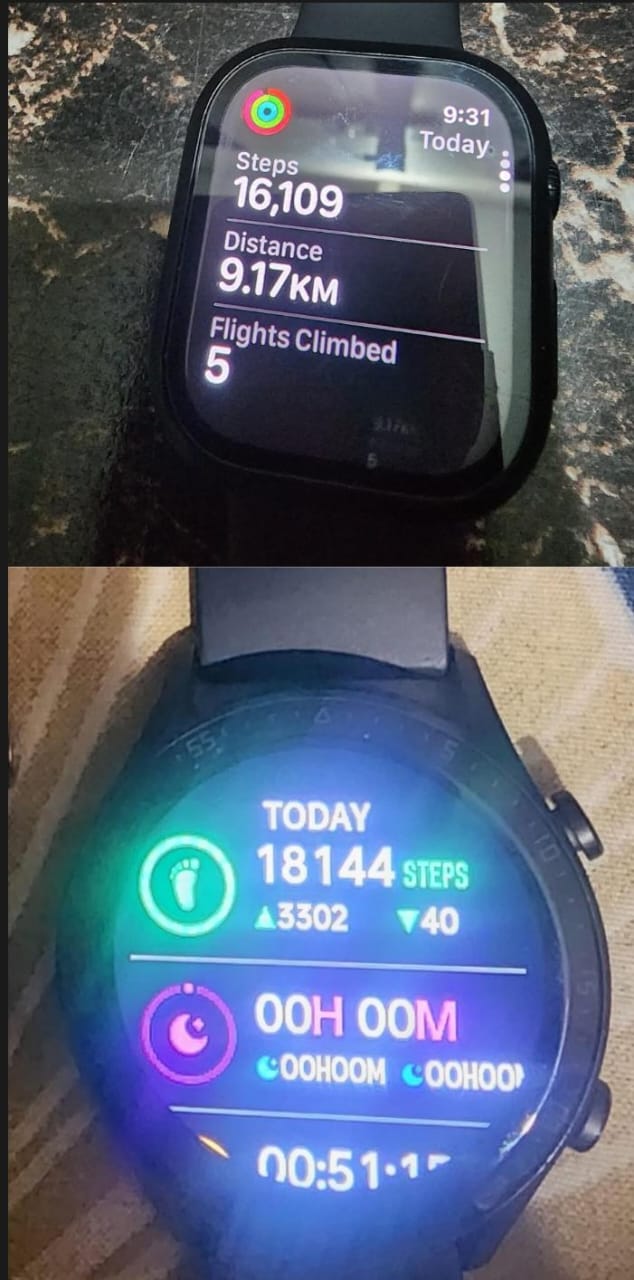
We started both of them at realistic step counts. When they joined, even 5,000 steps felt like a full day.
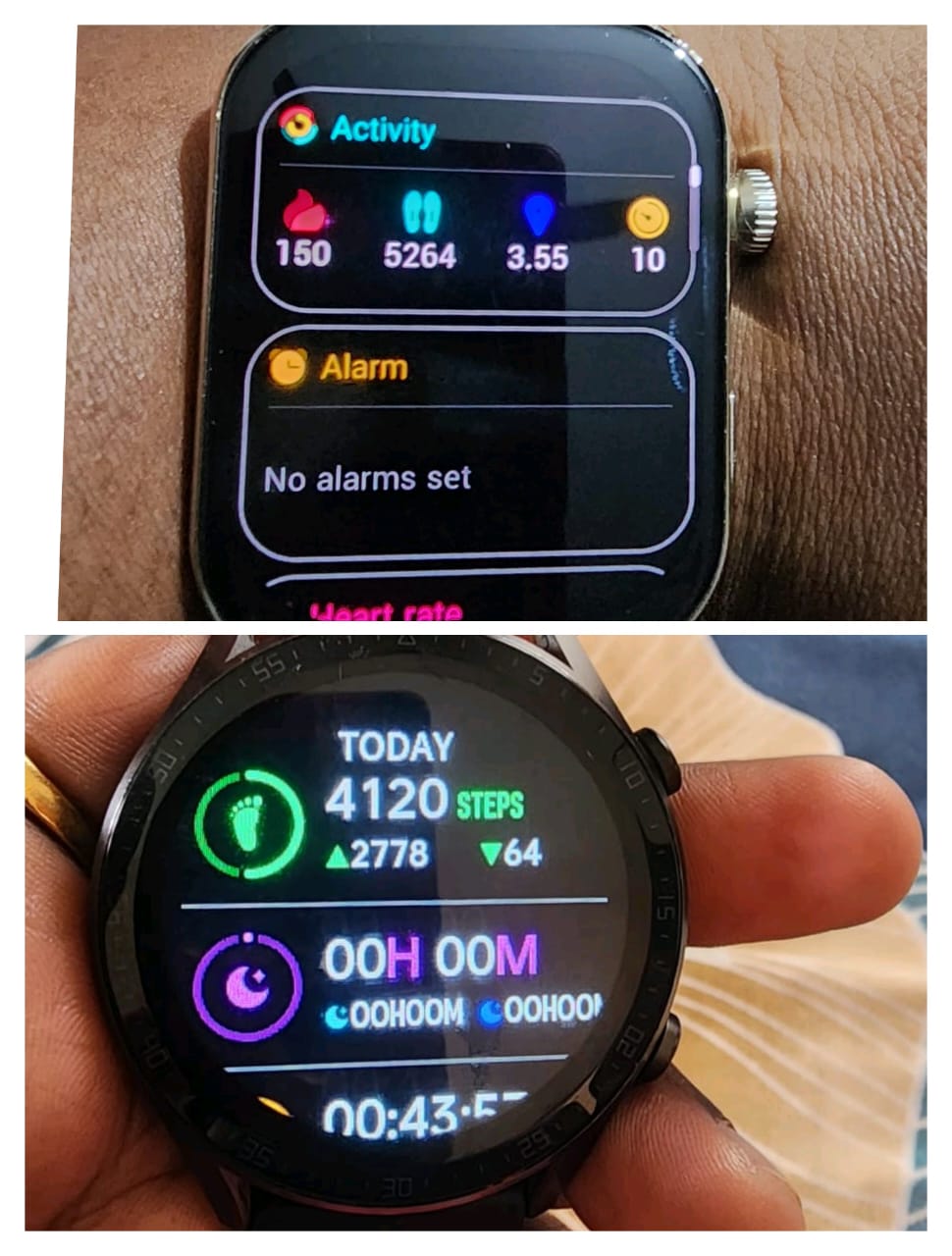
We moved the target up slowly, first to 8,000, then to 10,000. They walked during calls. They walked after meals (one of the most effective times for glucose regulation, particularly in Type 2 diabetes). They broke up sitting hours. They did not rely on motivation.

Over the months, 10,000 steps stopped being a target. It became a baseline. Some days they went past 15,000 without planning to.
Basic strength work was added gradually once walking was established, scaled to what Vivek’s cardiologist was comfortable with. No heroics. Small, repeatable sessions.
4. Routine correction before intensity
The less visible work was the most important. Meal timings got consistent. Sleep windows moved earlier. Late-night snacking stopped. Vivek’s work pattern, which had been the main reason his diabetes never settled, slowly stopped running his days.
We did not ask them to overhaul their lifestyle in a week. We asked them to do the same thing on Monday that they did on Sunday, and to keep doing it.
What Changed, Month by Month
The first three months saw the steepest drops on the scale. Both of them lost around 9 to 10 kg each. More importantly, the numbers on the inside started moving.
For Lalitha, the heavy bleeding reduced. Her cycles began to show a rhythm again. Her energy returned in a way she said she had almost forgotten. Her abdominal fat started to visibly reduce, and her thyroid began to stabilise.
For Vivek, the glucose pattern changed first. Fasting sugars came down. The post-meal spikes became smaller. His TSH, which had been 6.9, moved back into range. His CRP trended down week on week.


By month six, the transformation was obvious on every chart we had.
Lalitha: 118.3 kg to 99.8 kg (18.5 kg lost)

Vivek: 109 kg to 91.95 kg (17 kg lost)

The metabolic picture at six months
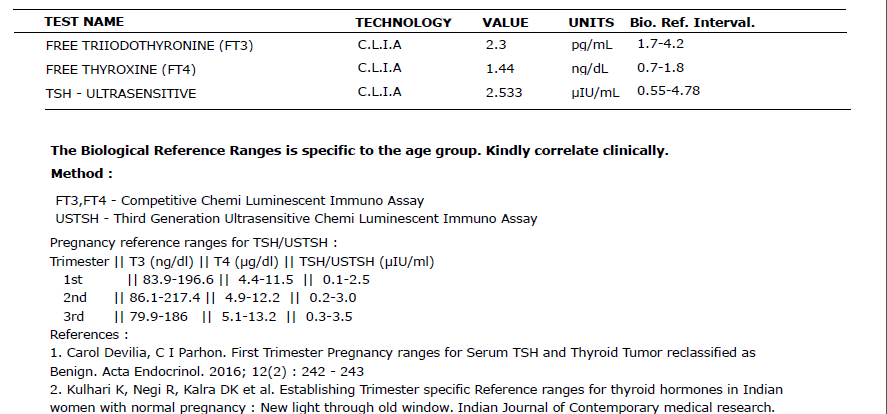
- Lalitha’s TSH: moved to 2.533 (close to the preconception target of under 2.5, with the trend heading right)
- Lalitha’s LDL cholesterol: optimised from elevated levels
- Lalitha’s inflammatory markers: reduced from the very high range
- Lalitha’s cycles: more rhythmic, less painful, less heavy
- Vivek’s blood sugar control: improved consistently (HbA1c trending down)
- Vivek’s TSH: back in normal range
- Vivek’s CRP: reduced meaningfully
Together, they had lost just over 35 kg as a couple.
Then the Pause
When it was finally time to move forward with IVF, something unexpected happened. Lalitha asked for one more month.
Not because anything was wrong. Not because her body was not ready. Because, after everything she had been carrying for years, actually standing at the edge of the procedure felt heavier than planning for it.
She had been told, more than once, that her egg reserve was low. She had been through two follicular studies where her ovaries had not responded the way anyone hoped. The idea that this time might be different was, in her words, harder to hold than the old familiar version of “this probably will not work.”
So she took the month. We did not add anything new. She kept doing what she had been doing for six months: the same plate, the same walks, the same morning routine. No extra pressure, no fresh protocol. Just steady consistency, the kind you build only by not breaking it.
And when the next cycle came, her body responded differently than it had before.
The Retrieval
Her stimulation cycle went better than any of her earlier follicular studies. Her ovaries responded. The retrieval was done successfully, and three embryos were formed and frozen.
For a woman who had been carrying the label of “low egg reserve” for years, three embryos is not a small number. In her context, it was a real, measurable, hopeful outcome.
This is what preparing the body does. It does not guarantee anything. It changes the odds.
They are now waiting for the embryo transfer. We will continue with them through that phase, the same way we went through the preparation: not stepping back after the good news, just staying alongside them.
The Results
| Metric | Lalitha (Before) | Lalitha (After) | Vivek (Before) | Vivek (After) |
|---|---|---|---|---|
| Weight | 118.3 kg | 99.8 kg (−18.5 kg) | 109 kg | 91.95 kg (−17 kg) |
| BMI | 50.5 (Obese III) | 42.6 (Obese III) | 37.3 (Obese II) | 31.4 (Obese I) |
| Fasting glucose | n/a | n/a | 153.3 mg/dL | Improved (trend down) |
| HbA1c | n/a | n/a | 6.8% | Improved |
| TSH | 4.24 (upper) | 2.533 (optimal) | 6.9 (high) | Back in range |
| hs-CRP | 22 mg/L | Reduced | 5.29 mg/L | Reduced |
| Vitamin D | 11.2 ng/mL (deficient) | Corrected | n/a | n/a |
| Cycles | Irregular, heavy | More rhythmic | n/a | n/a |
| IVF outcome | Low reserve label | 3 embryos frozen | n/a | n/a |
In Their Own Words
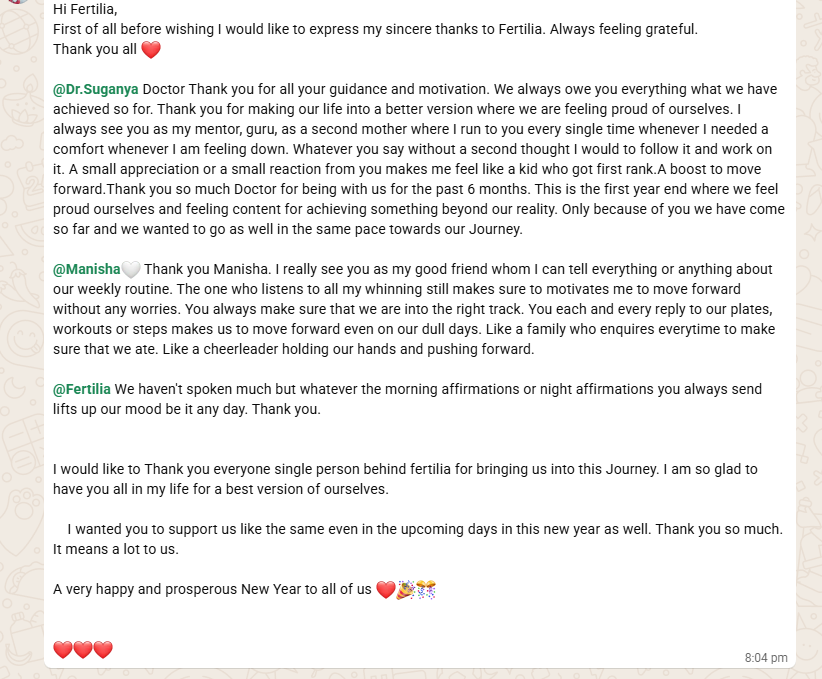
“First of all before wishing I would like to express my sincere thanks to Fertilia. Always feeling grateful. Thank you all.
@Dr. Suganya Doctor, thank you for all your guidance and motivation. We always owe you everything we have achieved so far. Thank you for making our life into a better version where we are feeling proud of ourselves. I always see you as my mentor, guru, as a second mother who I run to every single time whenever I need a comfort whenever I am feeling down. Whatever you say, without a second thought, I would follow it and work on it. A small appreciation or a small reaction from you makes me feel like a kid who got first rank. A boost to move forward.
Thank you so much Doctor for being with us for the past 6 months. This is the first year end where we feel proud of ourselves and feeling content for achieving something beyond our reality. Only because of you we have come so far and we wanted to go as well in the same pace towards our journey.
@Manisha, thank you Manisha. I really see you as my good friend whom I can tell everything or anything about our weekly routine. The one who listens to all my whinning still makes sure to move forward without any worries. You always make sure that we are into the right track. You each and every reply to our plates, workouts or steps makes us to move forward even on our dull days. Like a family who enquires every time to make sure that we ate. Like a cheerleader holding our hands and pushing forward.
I would like to thank everyone single person behind Fertilia for bringing us into this Journey. I am so glad to have you all in my life for a best version of ourselves.”
What This Story Teaches Us
1. Preparing the body does not compete with IVF. It supports it.
Lalitha and Vivek are not an example of lifestyle change replacing a medical procedure. They are an example of lifestyle change making the medical procedure more likely to work. The fertility specialist handles the stimulation, retrieval, and transfer. The program handles the metabolic environment the embryo will enter. Both matter. Neither is a substitute for the other. For the structured version of this kind of plan, see our 90-day IUI/IVF preparation guide.
2. A “low egg reserve” label is not a closing statement.
Ovarian response is shaped by more than a single AMH value or follicle count. Insulin sensitivity, thyroid status, inflammation, and weight all influence how the ovaries respond to stimulation. Correcting these before IVF is not wishful thinking, it is basic reproductive medicine. Lalitha’s three embryos, in the context she came with, is what happens when you give the ovaries a better environment to respond in. If you have been told your AMH is low, our guide on how to improve AMH levels naturally walks through what is and is not within reach.
3. Male metabolic health is part of the fertility plan.
Vivek’s cardiac history, diabetes, and central obesity were not separate from the fertility conversation. They were part of it. If a couple treats IVF preparation as only the woman’s project, they leave half of the biology unaddressed. This program changed because Vivek showed up too, every single day.
4. Consistency beats intensity, especially with a cardiac history.
None of what they did was dramatic. Walking. Portion control. Home food. Earlier bedtimes. Supplement correction. Steady check-ins. No extreme protocols, no risk to Vivek’s heart, no crash weight loss that would only rebound. Six months of the same things, repeated.
5. The emotional pause matters too.
When Lalitha asked for one more month, it was not weakness or avoidance. It was her body and mind needing to sync up before walking into the procedure. Good preparation makes room for that pause. Dismissing it would have pushed her in anxious; honouring it let her walk in steady.
Getting Ready for IVF? Let’s Build the Right Plan.
Every couple’s situation is different. Whether you are working through PCOS, managing diabetes, carrying a cardiac history, or simply want your bodies in the best possible place before the next step, we can help. We work alongside your fertility specialist, not in place of them.
Frequently Asked Questions
How long before IVF should we start preparing our bodies?
The evidence is strongest for a 3 to 6 month preparation window. Egg development takes roughly 90 days (Gougeon, 1986, Human Reproduction), sperm production takes about 74 days, and metabolic markers like HbA1c take 8 to 12 weeks to meaningfully shift. A 3 month preparation will help; a 6 month preparation, as Lalitha and Vivek did, gives both partners enough time to correct metabolic, hormonal, and inflammatory patterns, not just lose weight.
My AMH is low and I have been told my egg reserve is poor. Is preparation still worth it?
Yes, and often more so. AMH reflects quantity, not always quality. A healthier metabolic and hormonal environment, particularly stable thyroid, reduced inflammation, and improved insulin sensitivity, can change how the ovaries respond to stimulation even when the reserve number is low. Three embryos in Lalitha’s context is a real, meaningful outcome.
Does my partner need to do the same thing I am doing?
If your partner has metabolic issues (elevated blood sugar, high BMI, high blood pressure, thyroid dysfunction) or lifestyle factors that affect sperm (smoking, alcohol, chronic stress, poor sleep), yes, the preparation should be a couple’s project. Paternal metabolic health influences embryo quality, not just fertilisation (Campbell et al., 2015, Reproductive BioMedicine Online). IVF outcomes are a two-body story.
Vivek had a heart attack. Was it safe for him to lose this much weight?
The entire plan was designed around his cardiac history. No high-intensity cardio, no crash dieting, no aggressive fasting. Walking (a low-impact, high-benefit form of movement that actually reduces cardiac risk), gradual strength work scaled to his capacity, and a nutrient-adequate eating plan. Patients with coronary artery disease benefit from exactly this kind of steady, supervised weight loss (Ades et al., 2015, Mayo Clinic Proceedings). We also stayed in touch with the cardiology follow-up throughout.
Can you lose this much weight in 6 months safely?
A weight loss of 0.5 to 1 kg per week is considered a safe and sustainable rate. Lalitha and Vivek each lost roughly 0.7 kg per week on average over 6 months, right in the middle of that range. The key was that the weight came from consistent, nutrient-rich eating and daily walking, not from extreme restriction, so they did not lose muscle mass or micronutrient status in the process.
How does Fertilia work with our fertility specialist?
We work alongside, not instead. Your fertility doctor handles the medical side: stimulation protocol, monitoring, retrieval, transfer, medication. Our program handles the lifestyle side: personalised nutrition, movement, bloodwork-guided supplement support, daily check-ins, and routine correction. The two are complementary. Most of our patients continue to see their fertility specialist exactly as planned while working with us.
What if the embryo transfer does not succeed?
Then we continue with them. Preparation is not a one-shot contract. If a first transfer does not work, we keep the metabolic environment in a good place, review what can be optimised further, and support the next cycle. And if the medical path changes, for example moving from a fresh transfer to a frozen one, or adding additional testing, we adjust alongside that. The goal is that the body stays ready.
Do I need to be in Coimbatore to work with Fertilia?
No. Our program runs primarily through structured video consultations with Dr. Suganya, a nutritionist (Manisha or Elakiya), and ongoing WhatsApp check-ins. Most of our patients are outside Coimbatore, many are outside Tamil Nadu, and some are overseas. What you need is consistent internet and the willingness to share weekly updates.
Related Case Studies
- How Gowri went from HbA1c 9.8 to pregnancy. Gowri was referred to Fertilia by her gynaecologist for metabolic preparation before fertility treatment. PCOS, HbA1c 9.8%, BMI 38. She conceived in one cycle of ovulation induction after 3 months of preparation.
- How Madhu’s second embryo transfer succeeded. 30-day IVF preparation after a failed transfer: 6 kg down, fasting sugar normalised, transfer succeeded.
This is part of a series of real case studies from our clinic. Every story is verified and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.
Dr. Suganya Venkat is an OB-GYN with 15+ years of clinical experience. She holds a DNB in OB-GYN (GKNM Hospital, Coimbatore), an MD in Pathology (CMC Vellore), and an MBBS with 5 Gold Medals (SRMC).



