

Name has been changed to protect patient privacy. Clinical details and images are shared with the patient’s consent.
We usually talk about PCOS in the context of women in their twenties and thirties, navigating fertility, managing weight, or trying to regulate cycles after years of disruption.
But sometimes, the body sends its first signals much earlier.
This is one of those stories.
When It Started Early
She was 15. Harini was in her 10th standard, one of the most demanding academic years in the Indian school system, and most of her day looked the same: school, tuition, home, study.
She was tall for her age, 184 cm, and weighed 55 kg. On the outside, nothing looked unusual. Her body appeared lean and proportionate. But that lean appearance quietly masked something: her weight was on the lower side for her height and age, and her body wasn’t getting the nourishment it needed to function smoothly.
The routine made it harder. Long hours of sitting. The constant pressure of 10th standard preparation. And like many teenagers, her eating followed her hunger, not structure. When she felt hungry between study sessions, it was quick: chips, chocolate, an ice cream, a packaged snack. Not unusual for her age. Not even obviously wrong. Just a pattern that had settled in over time.
And then, slowly, her body began to show signs.
Her cycles started arriving late, or not arriving at all. Along with that came a low, persistent fatigue. Nothing dramatic, just a tiredness that didn’t quite match the day. She’d feel drained even on relatively quiet days, and neither she nor her parents quite understood why.
For a while, they waited. Hoping the next cycle would come on its own.
It didn’t.
When they took her in, she was diagnosed with polycystic ovaries.
The immediate suggestion was medication, hormonal tablets to bring the cycle. A reasonable clinical approach, especially in a busy outpatient setting.
But Harini’s mother wasn’t ready for that.
“My heart wasn’t ready to start her on medication so young.”
Starting a 15-year-old on hormonal tablets, for an indefinite period, felt like it was treating the symptom while leaving the real question unanswered. She wanted to understand what was actually happening inside her daughter’s body. And she wanted to know if there was another way.
That’s when they found Fertilia.
If your daughter or a young woman you know is showing signs of irregular periods or hormonal imbalance, it’s worth understanding what’s happening before reaching for a prescription. Start a conversation with Dr. Suganya on WhatsApp →
What the Assessment Revealed
The first thing we did was go through Harini’s reports carefully, not just the ultrasound, but the full picture.
Her ultrasound showed a polycystic ovarian pattern bilaterally: the characteristic finding associated with PCOS.
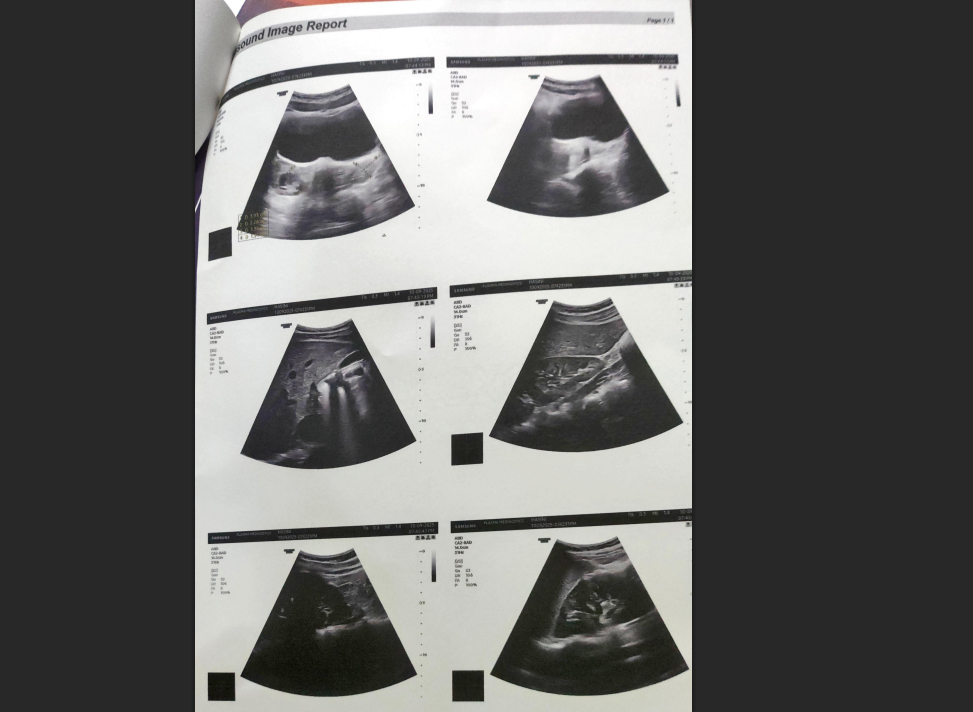
But what the ultrasound alone doesn’t tell you is why the body is presenting this way. For that, we needed to look deeper.
Her blood reports revealed two deficiencies that are extremely common in Indian teenagers, and almost always overlooked:
Vitamin D Deficiency
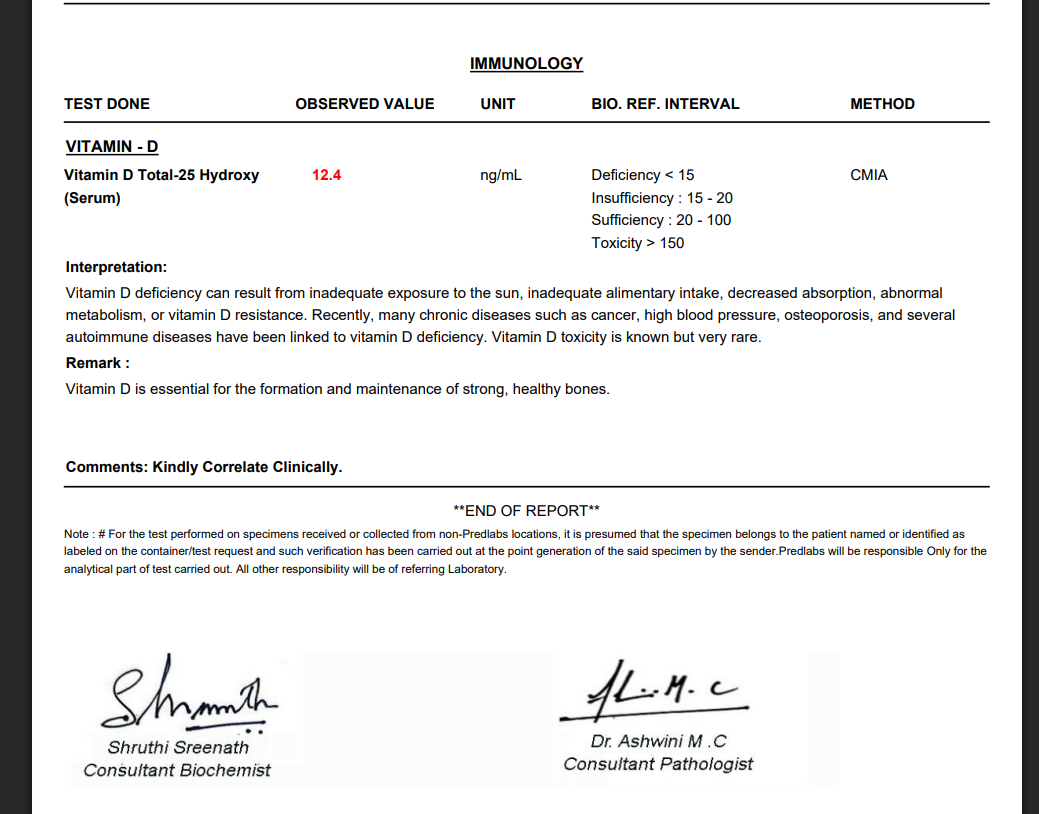
Vitamin D isn’t just a bone-health vitamin. It plays a direct role in hormonal signalling, insulin sensitivity, and ovarian function. A significant deficiency at this stage, during a period when the body is still maturing hormonally, can quietly disrupt the systems that keep cycles regular.
Vitamin B12 Deficiency
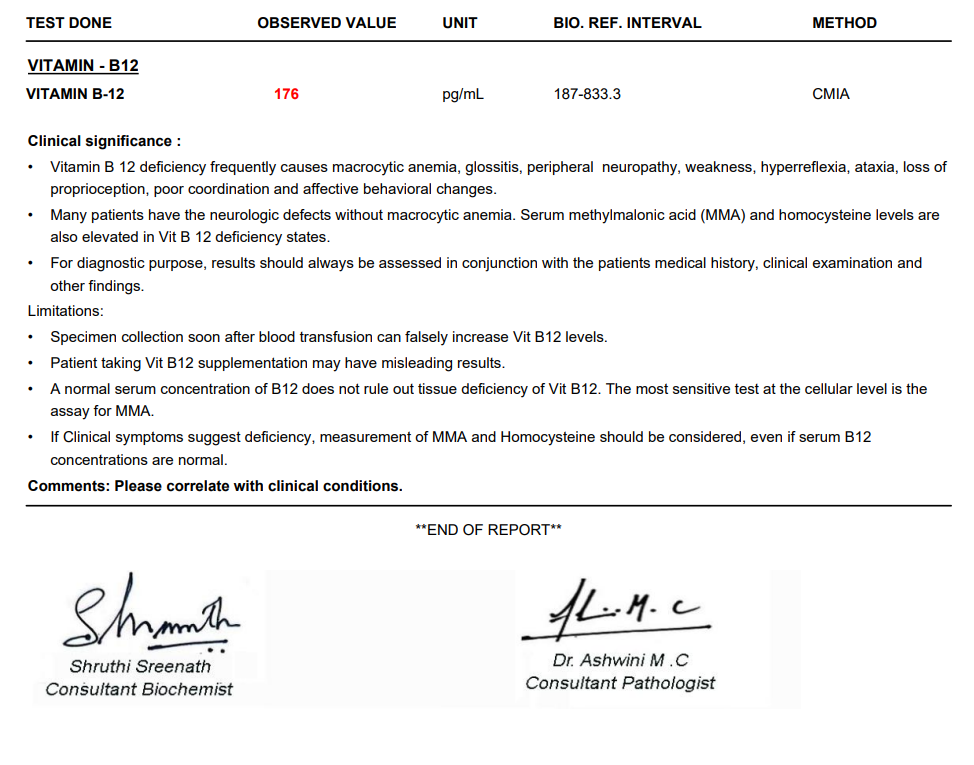
Vitamin B12 deficiency in teenagers is increasingly common, especially in those with limited protein intake. In Harini’s case, this was almost certainly contributing to the persistent fatigue she was experiencing. Low B12 slows down cellular energy production, leaving the body running on less than it should be.
Together, these findings painted a clear picture. This wasn’t a mystery. It was a body that had been under-resourced for a while, nutritional gaps, a sedentary pattern, academic stress, and was finally showing that in the form of disrupted cycles.
The question wasn’t whether this could be addressed through lifestyle. It was how to do it in a way that actually worked for a 15-year-old with a busy school schedule.
The Plan: Building a Foundation, Not a Restriction
The goal at this age was never to impose a strict diet or overwhelm Harini with a rigid programme. She was 15, in her 10th standard, managing academic pressure every day. Adding the stress of a complicated health protocol on top of that would have been counterproductive.
So we started with what her body actually needed.
Step 1: Correct what was deficient.
Before anything else, we focused on the clinical parameters. Targeted supplementation for Vitamin D and B12, appropriate for her age and deficiency levels. Not supplements piled on top of a broken foundation, but the actual foundation itself.
Step 2: Build her nutrition around her life.
Once the supplement piece was in place, we moved to food, and this is where Harini’s mother became essential. She was completely involved: tracking meals, sending daily updates, making sure the changes were followed with care at home.
We started by understanding what Harini liked to eat and what felt realistic within her routine. The goal was not restriction. It was redirection.
Instead of cutting out familiar foods, we introduced alternatives that felt natural to her, millets adapted in forms she was comfortable with, rather than forcing an entirely new diet overnight. Kambu aapam with egg omelette, jowar dosa with coriander chutney, ragi idly, jeera rice with rajma masala, PCOS-friendly Indian breakfast ideas adapted into school-friendly one-pot meals for weekdays, more structured eating when she was home.
![]()
Simple seed cycling was introduced alongside. Fruits were made non-negotiable. And spice-infused water, fennel water, fenugreek water, cinnamon water, became a consistent morning habit that her mother prepared at home.
One area needed gentle work: vegetables. Harini, like many teenagers, wasn’t particularly comfortable with them. We didn’t push. We started with what she was okay with and built from there at her pace.
The principle throughout was the same: make it simple enough that she could follow it without it feeling like a burden, and practical enough that a 10th standard student could actually stick to it.
Step 3: Introduce movement gradually.
Since Harini had been largely sedentary for months, we were careful not to overload her with an intense exercise routine. Movement was introduced slowly, following the same principles we use for all PCOS patients on what exercise actually helps. Some weekdays she managed it, some she didn’t. That was okay. But weekends were kept non-negotiable, to maintain consistency without creating pressure.
Over time, she found her rhythm.
What Changed. Month by Month
Month 1: Something Shifted
Harini followed the plan as consistently as a 10th standard student reasonably could. There were days when the school meal wasn’t ideal and she made do. There were evenings when exercise didn’t happen. But the overall direction was consistent, her mother tracked everything and shared daily updates.
And then came the message that changed everything.
Within one month of following the programme, Harini got her period naturally. Without a single tablet.
For more on this, read our guide on Lean PCOS. For a family that had been watching their daughter go through months of irregular cycles, and then facing the prospect of starting hormonal medication at 15, this was more than a medical milestone. It was relief.
Month 2: The Rhythm Continued
They didn’t change anything. Same food pattern, same movement, same daily tracking. Her mother stayed closely involved.
The result arrived again.
The second natural cycle. Around 32 days. No tablets. No intervention. Just her body, continuing to respond.
Month 3: Settling into Balance
By the third cycle, something quiet had settled in. Not just in Harini’s body, but in how her parents felt.
Three consecutive natural cycles. Aligned closely in timing. Her body was finding its own rhythm.
For her parents, who had spent months watching their daughter struggle with something she didn’t fully understand, quietly worrying about what it meant for her future, this was the reassurance they hadn’t dared hope for too soon.
In Their Own Words
Harini’s mother shared what this journey had meant to her:
And her father, in a Google review shared weeks after the programme:
A Note from Dr. Suganya: Why Adolescent PCOS Needs a Different Conversation
When a 15-year-old comes in with irregular cycles and a polycystic ovarian pattern on ultrasound, the first instinct in a busy outpatient setting is often to start a hormonal tablet to bring the period. I understand why. It works quickly, the cycle comes, and the visit ends on a reassuring note.
But for adolescents, this approach leaves the most important question unanswered: why is this happening?
Diagnosing PCOS in teenagers requires more care, not less. International guidelines are clear: in adolescents, irregular cycles alone are not sufficient to consider PCOS. The hormonal axis is still maturing in the first two years after the first period, some irregularity during this window is simply a normal part of that process. For PCOS to be considered in a teenager, we need persistent irregular cycles and clinical or biochemical evidence of elevated androgens, not one without the other. (Teede HJ et al., International evidence-based guideline for the assessment and management of polycystic ovary syndrome, 2018.)
That clinical caution matters. It means we should not over-diagnose, and we should not over-treat.
At the same time, when the picture is clear, a polycystic ovarian pattern on ultrasound, documented nutritional deficiencies, a sedentary lifestyle, and prolonged irregular cycles, it is equally important not to dismiss it or simply wait it out. Because the lifestyle foundation laid in adolescence has a long reach.
The metabolic drivers behind PCOS, insulin resistance, nutritional deficiencies, chronic sedentary patterns, don’t resolve on their own. When left unaddressed in the teenage years, they tend to deepen. Many women who come to me at 28 or 30 with longstanding PCOS trace their first symptoms back to 14 or 15. “I always had irregular periods, but everyone told me it was normal.”
The teenage years are a window. Establishing structured eating, correcting nutritional deficiencies, and building consistent movement at this stage is significantly easier than trying to undo years of disruption later in life.
In Harini’s case, we didn’t do anything aggressive or overwhelming. We corrected what was deficient, built a nutrition plan around her real life, and introduced movement at her pace. Her body responded quickly, because it had what it needed to find its own rhythm, and we simply gave it the support to do that.
If you have a teenage daughter with irregular cycles, especially alongside fatigue, weight changes, or skin symptoms, please don’t wait for it to “normalise on its own.” A proper assessment takes very little time. Understanding what’s driving it changes everything.
, Dr. Suganya Venkat, OB-GYN · 15+ years experience
What Harini’s Story Tells Every Parent
Adolescent PCOS is not a life sentence. It is a signal, one that, when addressed early with the right approach, responds beautifully.
A few things Harini’s journey makes clear:
Lean doesn’t mean nourished. At 55 kg and 184 cm, Harini looked fine on the outside. But her body was running on nutritional deficiencies that were directly affecting her hormonal function. Normal weight is not the same as adequate nourishment, and in teenagers, this distinction matters enormously.
Lifestyle-first can work before medication. In cases where the drivers are nutritional and activity-based, a food-first approach can restore natural cycles without hormonal dependency. This works best under proper medical supervision, not as a rejection of medicine, but as a structured alternative when the clinical picture supports it.
A mother’s involvement made everything possible. The daily tracking, the consistent updates, the willingness to adapt meals to what Harini would actually eat, without that level of involvement at home, the plan would have stayed theoretical. Harini’s transformation was a family effort.
Three cycles is a foundation. Harini’s story doesn’t end here. She’ll go through 11th and 12th standard, arguably the most stressful academic years in India. But she enters that period with a body in rhythm, a mother who understands how to support her, and the knowledge that her health is something she can actively take care of.
If your daughter is showing signs of irregular periods, fatigue, or hormonal imbalance, Dr. Suganya can help you understand what’s actually happening, and whether a lifestyle-based approach is the right first step. Talk to Dr. Suganya on WhatsApp →
Frequently Asked Questions
Can a 15-year-old have PCOS?
Yes, though diagnosing PCOS in adolescents requires more careful assessment than in adults. International guidelines (Teede et al., 2018) recommend that in teenagers, PCOS should only be considered when there is both persistent irregular cycles lasting more than two years after the first period and clinical or biochemical evidence of elevated androgens, such as acne, excess facial hair, or elevated androgen levels on blood tests. A polycystic ovarian appearance on ultrasound alone, in a teenager with irregular cycles, may simply reflect normal development. A proper clinical assessment is essential before a diagnosis is made.
How is adolescent PCOS different from adult PCOS?
The underlying hormonal disruptions can be similar, but the context is different. In adolescents, the hormonal axis is still maturing, some cycle irregularity in the first year or two after the first period can be completely normal. This makes the diagnostic bar appropriately higher for teenagers. At the same time, when true PCOS drivers are present, nutritional deficiencies, insulin resistance, sedentary patterns, elevated androgens, early intervention matters. The lifestyle foundations established (or not established) in adolescence shape what the condition looks like at 25 or 30.
For more on this, read our guide on From PCOS to Postpartum.
Is it safe to address adolescent PCOS without hormonal tablets?
In many cases, yes, when the underlying drivers are nutritional and lifestyle-based, and when the patient is under proper medical supervision. Harini’s case demonstrates what’s possible: correcting Vitamin D and B12 deficiencies, restructuring eating patterns, and introducing consistent movement brought three consecutive natural cycles without any hormonal medication. This approach is most effective when started with a thorough assessment, not independently of medical care, but as part of it.
Why did she have Vitamin D and B12 deficiency at 15?
Both deficiencies are extremely common in Indian teenagers, and both are frequently undetected. Vitamin D deficiency is widespread in India despite abundant sunshine, long sitting hours, indoor lifestyles, and minimal sun exposure mean most students aren’t producing adequate Vitamin D. Vitamin B12 deficiency is common in populations with limited animal protein intake. Both directly affect hormonal function, energy production, and metabolic health, making them important starting points in any assessment of irregular cycles in a teenager.
How quickly did her cycles return naturally?
Harini received her first natural period within one month of starting the programme. Her second cycle followed approximately 32 days later, and her third cycle came around the expected time after that. The speed of response reflects how significantly nutritional deficiencies were contributing as drivers, once corrected alongside structured eating and movement, her body responded relatively quickly.
What does a lifestyle-first approach for adolescent PCOS actually look like?
In Harini’s case: targeted supplementation to correct Vitamin D and B12 deficiencies, restructured meals using Indian foods she was comfortable with (kambu, jowar, ragi, jeera rice, home-cooked vegetables), consistent movement with weekends non-negotiable, and simple daily habits like seed cycling and spice-infused water. Her mother tracked meals daily and shared updates, that home involvement was central to what made it sustainable.
Should I get my teenage daughter tested if she has irregular periods?
If her periods have been irregular for more than one to two years after her first period, a proper assessment is worth doing. Blood work covering androgens, Vitamin D, Vitamin B12, and fasting insulin, alongside an ultrasound, gives you a clear picture of what is actually driving the irregularity. Many cases are entirely manageable with lifestyle changes once the specific drivers are identified. Early assessment and early action make the journey significantly easier.
This is the seventh in our series of patient case studies from our clinic. Every story is real, verified, and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.



