

Names have been changed to protect patient privacy. Clinical details and images are shared with the couple’s consent.
When most women hear “BMI and fertility,” they assume the conversation is about weight loss.
For Vidhya, it was the opposite.
She was 27, married for just over a year, working remotely, eating whenever her schedule allowed. From the outside, life looked stable. On the scale, it told a different story: 170 cm and 46.6 kg. BMI 16.1. That’s not “slim.” That’s moderate thinness on the WHO classification, the threshold below which the body starts conserving rather than thriving.
She and her husband Muruganathan, 28, a software engineer, had been trying to conceive for six months. Every month was the same loop, hope, then tears, then what’s wrong with me?
When she finally walked into Fertilia, she didn’t know that the question wasn’t only about her. It was about both of them. And it wasn’t only about food. It was about anxiety, ulcers, water, daylight, B12, and a marriage that needed to start moving in the same direction.
This is her story.
”I Eat… I Just Don’t Eat Properly”
The first consultation didn’t feel like a hospital visit. It felt like a long conversation, the kind no one had taken the time to have with her before.
She talked about her routine, the work-from-home schedule that meant breakfast at 11, lunch at 4, dinner sometimes at 11 pm. About her ulcers and gastritis that flared every time she ate spicy food. About a recent dental procedure that had left her with persistent throat irritation, so eating felt uncomfortable. About how little water she drank, “maybe two glasses a day, sometimes one”.
And then she said the thing many underweight women say, almost as a confession:
“I eat… I just don’t eat properly.”
That sentence carries a whole world inside it. It means: I’m not anorexic. I’m not refusing food. I’m just busy, irritated, anxious, distracted, and food keeps slipping to the bottom of the list. By the time she remembers to eat, it’s something quick, something safe for her stomach, something small.
For her body, that pattern translated into one message: we are not in a season of abundance.
A body that doesn’t feel safe doesn’t prioritise reproduction. That’s not a moral judgement. That’s biology. Reproduction is metabolically expensive. When energy intake is unreliable for months on end, the body quietly down-regulates the systems that aren’t immediately essential, and ovulation is one of the first to go on a low setting.
This is what people miss when they hear “BMI and fertility.” They picture extremes. The reality, in clinic, is far more common: a busy young woman, a normal-looking life, and a quietly underweight body that has stopped trusting the next meal will come.
The Anxiety Layer Underneath
Then there was the part Vidhya didn’t write down on her intake form, but that came up within the first ten minutes of conversation.
She was an anxious person. She always had been. Small things felt overwhelming. Big things felt unbearable. And every cycle of trying to conceive had a particular rhythm to it: a few days of cautious hope around ovulation, two weeks of intensive symptom-spotting, and then the heart-sinking moment her period arrived.
“I would worry every month. The whole cycle, I’d be tense. Then when my period came, I would cry.”
This is one of the most under-discussed parts of fertility. The cumulative emotional weight of trying-and-not-succeeding, month after month, is a clinical issue, not a personality flaw. Chronic stress and anxiety affect cortisol, which affects insulin and reproductive hormones. Anxious eating affects digestion, which affects nutrient absorption. Poor sleep, which almost always accompanies anxiety, affects everything.
A holistic plan that ignores this layer rarely works. We knew from the start that her plan needed to include the emotional architecture, not just the food and supplements.
Going Deeper: Both Partners’ Reports Told a Story
When the test results came back, the picture clarified.
Vidhya’s Vitamin D and B12
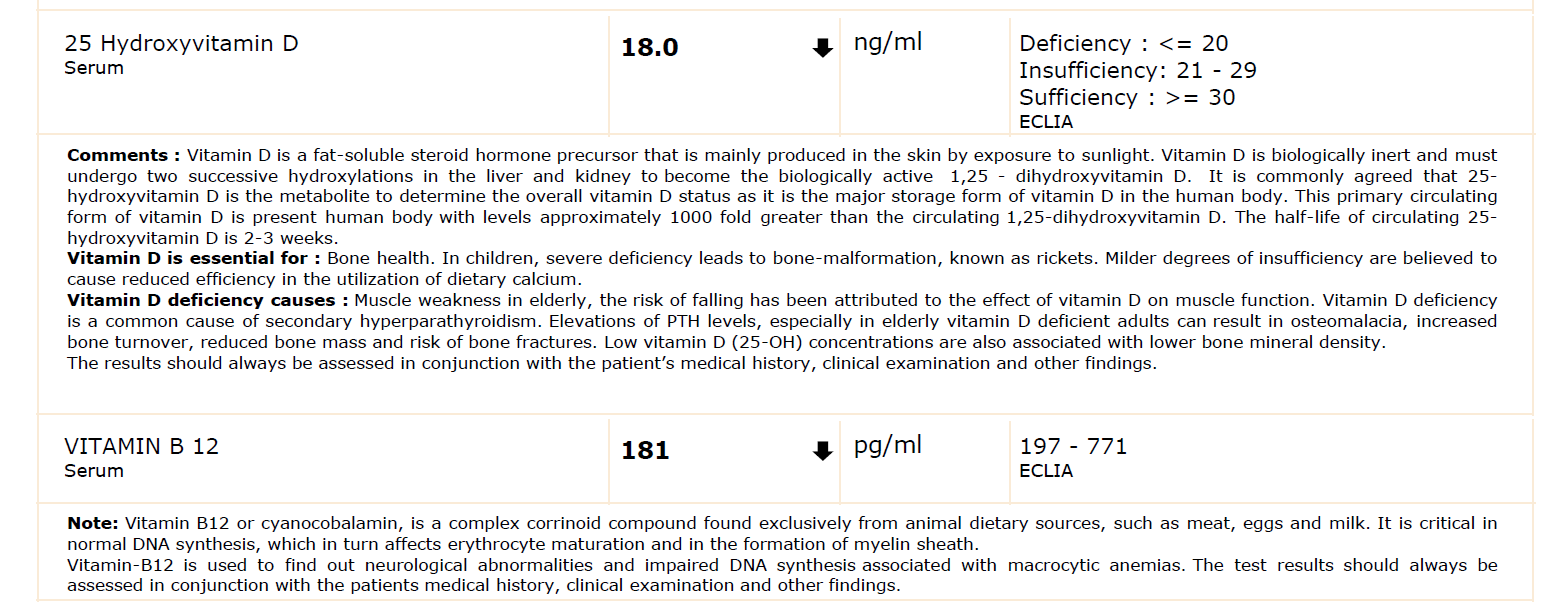
Her Vitamin D was 18 ng/ml, in the deficiency range (≤20). Her B12 was 181 pg/ml, below the lower limit of the reference range (197–771).
Both deficiencies are extremely common in Indian women, especially those who spend most of their day indoors and don’t eat large amounts of animal protein. They also matter more for fertility than most women are told.
- Vitamin D plays a documented role in ovarian follicular development and endometrial receptivity. Deficiency has been associated with poorer outcomes in both natural and assisted conception.
- Vitamin B12 is essential for DNA synthesis and red blood cell formation, and works alongside folate in the same one-carbon metabolism pathway that supports egg quality and early pregnancy.
These weren’t “small numbers.” They were foundational.
Muruganathan’s Vitamin D and B12
What surprised the couple was the next set of reports.
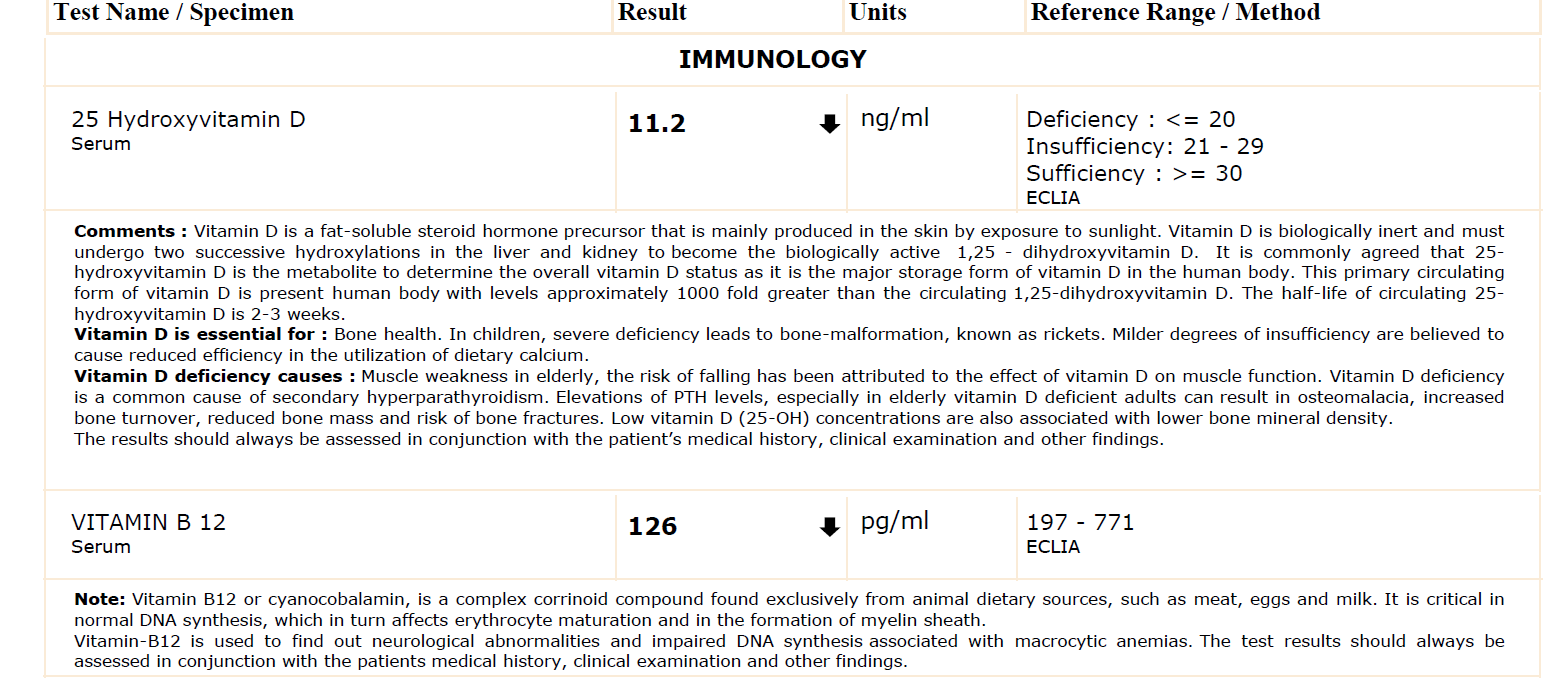
Muruganathan’s Vitamin D was 11.2 ng/ml. His B12 was 126 pg/ml. Both were lower than his wife’s.
This is a part of fertility that almost never gets addressed in routine consultations. The default assumption, especially in Indian clinical settings, is that “trying to conceive” is a women’s-health appointment. The man comes along, sometimes provides a semen analysis, and otherwise stays in the background.
But conception is a 50-50 contribution. Sperm quality, motility, and DNA integrity are directly affected by paternal nutrient status, especially Vitamin D, B12, folate, zinc, and omega-3 levels. A man whose own foundational labs are deficient is contributing his half of the puzzle from a depleted base.
We see this often, and it’s why our assessment looks at both partners. A 90-day program for the woman alone, while the husband continues his existing routine, leaves half the equation untouched.
For more on the male side of this picture, our Male Factor Infertility case study walks through a different couple where this turned out to be the main story.
Vidhya’s BMI Profile
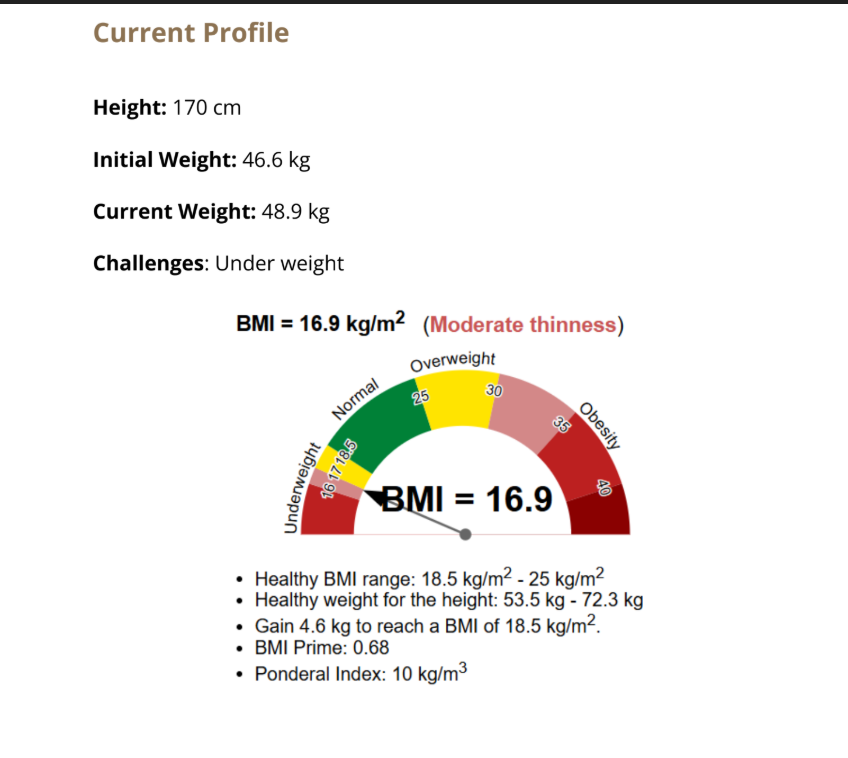
Her starting BMI was just above 16. The healthy range starts at 18.5. To reach the lower end of healthy, she would need to gain at least 7 kg, not in a rush, but steadily. The number itself wasn’t the goal. Restoring the body’s sense of nutritional safety was.
We brought all of this together in one frame for the couple: both of you have foundations to rebuild. Let’s not rush a result. Let’s rebuild the floor first.
This reframe mattered. For the first time in months, the conversation wasn’t what’s wrong with me. It was here’s exactly what we’re working on, both of us, together.
If you’re TTC and feeling like no one has asked the right questions about your nutrition, your husband’s health, or what’s actually going on in your body, Dr. Suganya can help. Talk to Dr. Suganya on WhatsApp →
The Plan: Build Before Expecting
Foundation Phase: Correct What Was Missing
Before anything else, both partners started clinically appropriate supplementation:
- Vidhya: Vitamin D correction targeted to move her from 18 to above 30, active B12 supplementation, and additional support for her ulcer-related digestion.
- Muruganathan: Higher-dose Vitamin D correction (he was more deficient), B12, and basic preconception nutrient support including folate and zinc.
Supplements alone were never the strategy. They were the floor. The lifestyle changes built the walls.
A Diet That Changed Every Month
Vidhya’s diet plan wasn’t fixed. It was rewritten every month based on how her body was responding, what her digestion was tolerating, and what her energy levels needed at that stage.
The principles stayed constant:
- Calorie-dense and nutrient-dense, not just calorie-heavy. An underweight woman with ulcers and gastritis cannot just “eat more.” She has to eat the right kind of more.
- Gentle on her gut. Her ulcer and gastritis history meant we explicitly avoided anything that triggered her, even if a “PCOS-friendly” or “fertility-friendly” food list elsewhere might recommend it. The food that helps you must also be food you can digest.
- Spread across the day. Five smaller meals worked better for her than three larger ones. Smaller portions meant less digestive distress and better absorption.
- Anchor protein in every meal. This is non-negotiable for an underweight body. Eggs, fish, paneer, dal, curd. (For more on how to think about this practically, see our PCOS Diet Chart, the protein principle is the same regardless of diagnosis.)
Here’s what some of her plates looked like once the routine settled:



Notice what these plates have in common: a complete carbohydrate, a real protein source, a vegetable, and dahi or chutney. Nothing fancy. Nothing imported. Nothing she had to learn from scratch. Just structured, intentional Indian meals, eaten on time.
The Hydration Reset
We also addressed her water intake, quietly the most under-rated lever in everyday Indian women’s health.
She was drinking 1-2 glasses a day. We started with a single goal: a glass of water within 10 minutes of waking up, before tea. Then a glass before lunch. Then a glass mid-afternoon. Within three weeks she was at 6-8 glasses without it feeling like a chore. Her ulcer flare-ups settled noticeably with this single change.
Movement, Together
This is the part that turned out to matter more than we expected.
We didn’t ask her to start a workout programme. She was underweight, anxious, and already feeling overwhelmed. Pushing intense exercise on a body in deficit would have backfired.
Instead, we introduced gentle, paired movement. Both of them. Together. Walking after dinner. A short stretching routine in the morning. Some basic strength movements twice a week. Nothing intense. Nothing she’d dread. Just enough to support circulation, sleep, and mood.
What surprised her was how quickly this became their time. Muruganathan, who had his own foundational deficiencies to address, began to share the routine with her. The walks turned into conversations. The morning stretches became a small ritual that bookended the day.
This is one of the most under-rated parts of a fertility journey: when both partners move together, the woman stops feeling like she’s the project. That single shift, from I’m being fixed to we’re working on this together, changes everything about how a woman experiences her own treatment.
The Journey: Slowly, Then All At Once
The changes came gradually, the way real changes do.
Weeks 1-4: Steady Inputs, Steady Doubts
In the first month, she did everything she was asked to. Supplements, every day. Five small meals, most days. Water, slowly increasing. Walks, when she could. There were also days when she couldn’t, and she let those go without spiralling.
But the anxiety didn’t switch off. There were nights she lay awake worrying about whether her cycle would come on time, whether the plan would work, whether she was somehow not doing enough.
We expected this. So did she. The worry didn’t mean the plan was failing. It meant she was the same person, doing something new.
One-Month Update: The First Reassuring Numbers
A month in, we measured.
She had moved from 46.6 kg to 48.9 kg. Just over 2 kg in 30 days. Not dramatic. Exactly what we wanted. Sustainable weight gain in an underweight body is slow weight gain. Anything faster usually means fluid, poor-quality muscle, or bingeing, none of which serves fertility.
More importantly, her ulcer symptoms had begun to settle. The throat irritation was easing. Her water intake had stabilised. Sleep was a little better.
This is the moment that quietly turns a patient from sceptical to engaged. Numbers on a scale don’t do it. Symptom relief does. When her ulcer started settling, when her energy stopped crashing every afternoon, she felt, for the first time in months, that her body was cooperating with her again.
Mid-Program: The Check-In That Changed the Tone
A few weeks later, she sent her weekly check-in:
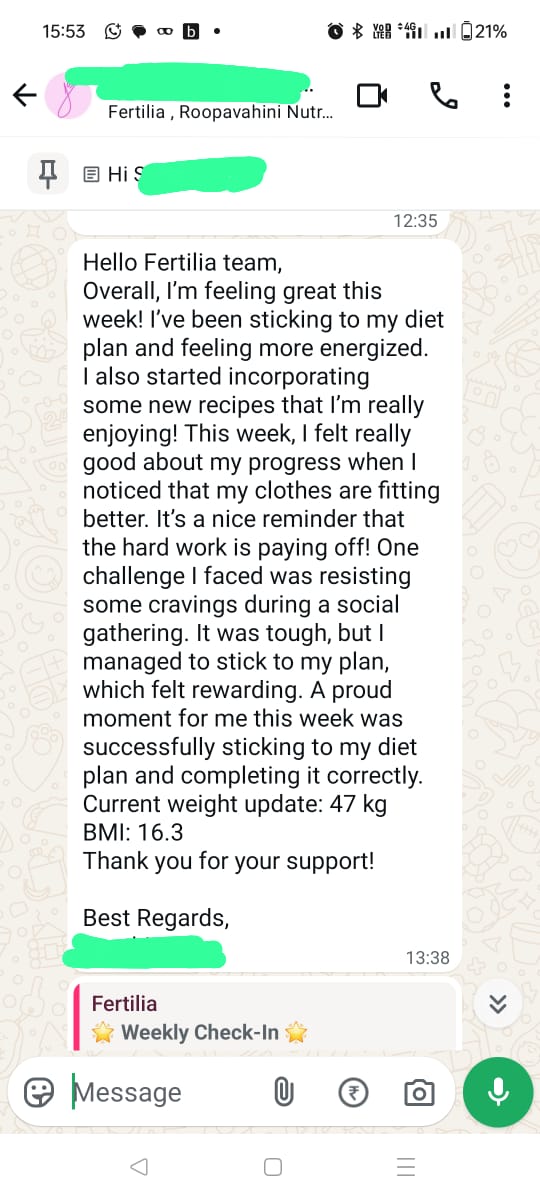
What’s worth noticing in this message isn’t just the weight update. It’s the tone. A few weeks earlier she had been worrying her way through every cycle. Now she was sending a list of small wins, I felt energised. My clothes fit better. I held my plan at a social gathering. The shift from anxious to engaged had started.
This is what we mean when we say a fertility plan is also a confidence plan. The same woman, same body, same household, was now narrating her own progress instead of waiting for someone to tell her if she was doing it right.
Months 2-3: Settling Into a Lifestyle
By the second month, the routine had stopped feeling like a programme. It was just what they did now. Both of them.
Periods came. Periods went. There was still some disappointment around each cycle, that doesn’t disappear quickly. But the shape of the disappointment changed. It wasn’t what’s wrong with me. It was we’ll keep going.
Her weight kept climbing slowly. Her digestion kept improving. Muruganathan’s energy levels noticeably picked up too, which neither of them had been expecting.
The Choice After the Program Ended
At the end of the 90-day program, she had not yet conceived.
This is the moment that defines whether a woman is going to look back on the program as worth it. Many women, at this point, lose the structure and slide back into old habits. The supplements get skipped. The plates get smaller again. The walks get shorter.
Vidhya did the opposite. She kept going.
For the next three to four months, without a structured program around her, she continued the same lifestyle, on her own. Five meals. Adequate water. Walks with her husband. Supplements where they were still needed. Plates that looked like the ones above.
And then, one quiet morning, the test came back positive.

A few days later, the early ultrasound confirmed an intrauterine pregnancy.
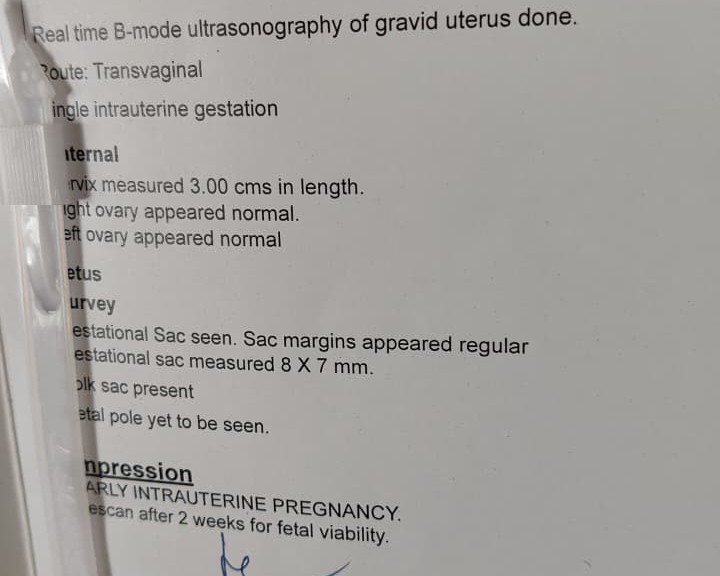
A single intrauterine gestation. Both ovaries normal. Yolk sac present. The earliest unmistakable confirmation that everything had landed where it was meant to.
She conceived naturally, without IUI, without IVF, without ovulation-induction medication. Just a body that had finally been given enough time, food, water, sleep, partnership, and patience to do what it had always been capable of doing.
In Her Own Words
After the positive test, she sent a long message. We’ve shared it with her permission.
The lines that matter most in that message aren’t the result. They’re these:
“What made the biggest difference was that we started doing everything together.”
“Even after the official 3-month program ended, we continued the same diet and exercise pattern because we genuinely felt better.”
Those two sentences carry the entire framework of how this case worked.
Why Low BMI Affects Fertility, And Why It’s Often Missed
Most fertility content, on Instagram, in clinics, in popular books, focuses on the woman who is overweight or has PCOS. The advice almost always goes one direction: lose weight to improve your chances.
That advice, when it applies, is correct. But it leaves an entire group of women invisible: women like Vidhya, who are underweight, often busy, often anxious, often eating less than their bodies need without realising it.
Here is what research has consistently shown:
- Both ends of the BMI spectrum reduce conception rates. A landmark Danish prospective cohort study of more than 2,500 couples found that women with a BMI under 18.5 took significantly longer to conceive than women with a BMI in the 20-25 range, with fecundability ratios reduced for both underweight and obese categories (Wise et al., Hum Reprod, 2010).
- Underweight women have higher rates of menstrual irregularity, anovulation, and luteal phase defects (ESHRE Capri Workshop Group, 2006). The mechanism is hypothalamic, when energy availability is low, the hypothalamus reduces GnRH pulsatility, which reduces LH and FSH signalling, which affects ovulation.
- The optimal BMI for natural conception sits in the range 20-25, with the lowest fecundability decline reported in this band across multiple cohorts.
This is the science. The clinical reality, however, is that an underweight woman is far less likely to be told this clearly. She’s far more likely to be reassured that “you don’t need to lose weight, you’ll be fine,” and sent home without a structured plan to address why her body isn’t ovulating reliably.
Optimal BMI is not a vanity metric. It’s a fertility metric. Restoring it, gently, sustainably, with the right protein and the right calories, is one of the most under-rated interventions in modern preconception care.
What This Case Reinforces
There are three things this couple’s journey makes plainer than usual.
1. Both Partners Need to Be Assessed
Conception is a 50-50 contribution. Yet most TTC consultations treat the woman as the patient and the man as a bystander. If a man’s Vitamin D is 11.2 and his B12 is 126, that is going to affect sperm quality regardless of how perfectly his wife follows her plan. Couples who get assessed together, supplemented together, and changed lifestyle together tend to convert that into outcomes faster.
2. The Lifestyle Has to Outlast the Program
Vidhya did not conceive in Month 3. She conceived after she kept going for another three to four months on her own. Healing happens on the body’s timeline, not the calendar’s. A 90-day program is the period when the structure is held externally. The job, by the end, is to make the lifestyle so familiar that you don’t need the structure anymore. That’s what gives the body the runway it needs to do something it hasn’t been able to do for a long time.
If you want to read about another patient who kept going past her formal program, our How Nisha Reversed Her PCOS case study has the same arc.
3. The Couple Has to Travel Together
The single most important sentence Vidhya wrote in her testimonial wasn’t about food. It was: “we started doing everything together.” The walks. The meals. The supplements. The check-ins. The sense of we’re in this.
An anxious woman, going through a TTC journey alone while her husband watches from the sidelines, has a much harder body chemistry to work with than the same woman whose husband is walking with her after dinner and taking his own supplements alongside hers. Fertility is a household-level project, not an individual-level one.
Trust Your Body. Build the Support System. Travel the Journey Together.
That’s the line Dr. Suganya keeps coming back to with couples like Vidhya and Muruganathan.
Trust your body. It is not broken. It is responding to the conditions you give it. When the conditions change, the response changes.
Build the support system. The husband is not optional. The food at home is not optional. The water you drink is not optional. The way you talk to yourself in the difficult weeks is not optional.
Travel the journey together. Not just for the official 90 days. For as long as it takes.
The results, in their time, follow.
If you’re TTC and your BMI is on the lower side, or you’ve been told “you’re fine, just keep trying,” it may be worth a deeper look. Dr. Suganya works with couples one on one, starting with a full assessment of both partners. Start a conversation with Dr. Suganya on WhatsApp →
Frequently Asked Questions
Can low BMI affect fertility?
Yes. Multiple large prospective studies (including Wise et al. 2010 in Human Reproduction) have found that women with a BMI under 18.5 have lower per-cycle conception rates and longer time-to-pregnancy than women with a BMI in the healthy range. The mechanism is hypothalamic: when calorie availability drops, the hypothalamus reduces the hormonal signalling that drives ovulation, leading to irregular cycles, anovulation, and luteal phase defects.
What is the optimal BMI for conception?
Most fertility research consistently points to a BMI of around 20-25 as the range associated with the highest natural fecundability. Below 18.5, the body’s hormonal signalling is suppressed; above 30, insulin resistance and inflammation start to interfere. The exact “best” number varies by individual, but for most women, working towards the 20-23 band is a reasonable preconception goal.
How long does it take to conceive after correcting underweight?
It varies. The body needs time to register that energy supply is reliable before it restores ovulatory regularity. In practice, we often see meaningful cycle and energy improvements within 1-2 months of consistent nutritional correction, but conception itself may take an additional 3-6 months as the reproductive axis fully re-establishes. Vidhya conceived approximately 6-7 months after starting structured changes, three months in the program, three to four more months continuing the same lifestyle.
Do men’s Vitamin D and B12 levels affect fertility too?
Yes. Sperm quality, motility, and DNA integrity are directly affected by paternal nutrient status. Vitamin D is involved in sperm membrane function and motility. B12 supports DNA synthesis and is essential for healthy sperm production. Folate, zinc, selenium, and omega-3 levels matter too. A man whose foundational labs are deficient, especially when his wife is also deficient, contributes his half of the equation from a depleted base. Couples who get assessed and supplemented together tend to see results faster.
Can anxiety actually affect getting pregnant?
Anxiety doesn’t directly “block” conception, but chronic stress and anxiety influence cortisol, sleep quality, digestion (and therefore nutrient absorption), and the menstrual cycle through the HPA-HPG axis. Long-running anxiety also affects how a woman eats, often less reliably and less frequently, which compounds the nutritional issues. Addressing the emotional layer is part of the plan, not a separate concern.
How fast should I gain weight if I’m underweight and trying to conceive?
Slowly and steadily. A reasonable target is around 0.5 to 1 kg per month through nutrient-dense food, not through “eating more of anything.” Rapid weight gain often comes from fluid retention or low-quality calories, neither of which serves fertility. Sustainable gain, with adequate protein, healthy fats, and complex carbohydrates, is what restores the body’s hormonal stability.
Is low BMI common in Indian women trying to conceive?
It’s more common than people realise, especially in young, urban, working women whose schedules push meals to irregular times. National surveys (including India’s NFHS-5) have repeatedly found a significant proportion of women in the underweight category, despite the simultaneous rise of obesity. In our clinic, lean and underweight presentations show up in fertility consultations more often than the typical “PCOS narrative” of the internet would suggest.
Should I see a doctor for low BMI fertility issues, or just try to gain weight on my own?
A proper assessment matters. As Vidhya’s case shows, low BMI is rarely just “low BMI.” It usually comes packaged with vitamin and mineral deficiencies, sometimes a digestive condition (ulcers, gastritis, IBS), often anxiety, and frequently a partner whose own foundational labs haven’t been checked. Trying to “just eat more” without addressing those layers tends to fail. A structured plan, ideally one that includes both partners, gives the body the conditions it actually needs.
This is part of our Real Stories series, detailed patient case studies from Dr. Suganya’s clinic. Every story is real, verified, and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.



